Life Expectancy
I have often complained that reliance on the gross life expectancy numbers in the health care debate can be misleading. Life expectancy is a function of a number of variables of which health care is but one (in fact we could even break health care down into several variables such as access to care, quality of care, etc.). Greg Mankiw has found an interesting blog post at Carpe Diem that looks at actual life expectancies and standardized life expectancies (i.e. corrects for non-health care deaths such as homicides and car accidents).
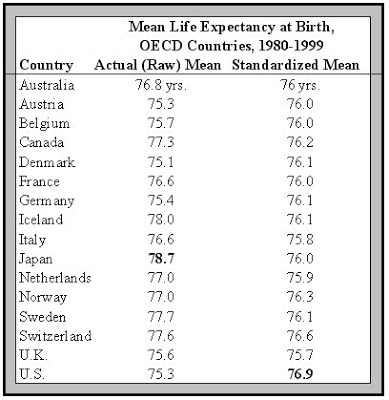
Now the study in question is not much more than a presentation, so take the above numbers with a grain of salt. However, the study is asking the right question: if we control for things like homicides, car accidents and other forms of non-health care related premature deaths how does the U.S. life expectancy rank?
“I intend to live forever, so far so good.” — Steven Wright
How is it that the life expectancies in other countries drops when “non-healthcare” related fatalities are removed?
Are a negative number of Japanese murdered each year?
This chart doesn’t make any sense at all. There is no supporting information in the linked blog post or even the pdf presentation that it is taken from.
It wouldn’t have to be murders, just accidental via falls, car accidents. If Japan had to remove a number of data points that died accidentally above the mean then the number would go down for health-care related (or natural) causes. Presumably all accidental, murder, etc cases would be removed both above and below the mean in all countries, because you wouldn’t know how to count them against the standardized category.
No, it only makes sense to remove accidental deaths/homicides before the median age. It makes perfect sense that the median lifespan would go up for America, given our high murder and auto accident rates. However, for other countries where, I suppose, a surprising number of old people die in accidents, they have survived to older than median age probably in some part to the healthcare they have received.
The methodology that you propose does not make any sense, but we still don’t know what methodology the study uses.
Also, there would have to be an insanely large amount of old people dying in accidents to cause a multi-year drop in median age, so the numbers themselves seem fishy.
and it is happening in 10 of the 16 countries listed.
Must be lots of fatal slip and fall accidents among the elderly in Canada and the EU. It’s really bad in Iceland. Maybe we should be sending them some of those sticky mats for their showers.
What doesn’t make sense is to remove only part of the accidental death data (below the median age). First of all this changes the median age so where do you stop. You can only remove all the accidental death data because you don’t know the impact against natural cause death from any accidental death datapoint. If someone is 80 and dies accidently you don’t know if he/she would’ve lived to 90 or 100, just like you don’t know if someone that dies accidently at 40 wouldn’t have lived to 110. You either have to remove all the accidental deaths or none of them or you then really ARE skewing the data and making it statistically insignificant. Ask a statistician.
Obviously anyone living past the median age then dying of an accident would’ve otherwise increased the median, but leaving them in the pool only contaminates the data.
Just as a side note, I didn’t propose any methodology, I just reversed engineered what must have been used, base on the data anomaly you mentioned and what little I know of data collection and statistics.
The question was “…how does the U.S. life expectancy rank?” I respond, pretty damn well. For whatever variables anybody wishes to include or remove, the USA is always near the top in life expectancy. The highest (few) countries are always in the low-80s, and we’re always in the mid-to-high 70s. Considering our high stress level and rich food intake, we’re doing great. I’ll keep all my toys (stress-induced work to get them all) and protein/fat-rich foods and live a few less miserable years as an elderly person.
Adam: what we don’t do well at is price/performace with respect to healthcare.
Even if the “standardized mean” values are correct, that means we’re getting an average of 1-2 years of extra life by spending twice as much, per person, on healthcare than do the other western nations.
rodney: The reason that you take out accidents when you’re trying to measure lifespan wrt healthcare is that they are generally not related to health or healthcare. However, living past the median age probably is highly related to healthcare, so whether or not you die of an accident or cancer at age 85 means that healthcare was significant.
So, in summary, I think the supposed methodology doesn’t make sense, the numbers look screwy anyway, and it’s not impressive even if it were true.
Oh I understand why you take out the accidents, you just can’t take some out and leave others in without corrupting the statistical model.
I agree that living past the median, then dying of an accident is significant, it just can’t be use is the model, as you can’t tell how significant it is. (and is obviously why the Japanese and Icelandic numbers went down).
It is also significant from a healthcare perpective when someone dies of an accident at age 30, when they otherwise would’ve died of a heart attack at age 45. You just have no way of telling this, just as you don’t know that someone who dies at 85 of an accident could have lived to 110 otherwise. You can’t mix in some of the accidental deaths and still have a clean data model.
The methodology makes absolute sense statistically and yes it does make the numbers look screwy.
However, It does mean ‘something’. If Japan and Iceland for example can decrease accidental deaths of their elderly their standardized mean would increase significantly.
Perhaps this is an example of supply-side demographics. Increase the murder rate and longevity increases as well!
Actually it does if you want to look at the effects of health care on life expectancy. You’d want to remove all premature deaths due to factors other than those relating to health care.
Yes, you sure do get lots of performance for the price by putting people on a waiting list for 16 weeks.
When will you stop using this blatantly misleading argument as your primary response to lower prices in other nations? Out of dozens 1 possibly 2 have waiting lists that approach this length and then only for specific proceedures. No serious person is suggesting we follow the UK model so you should just stop this particular misdirection of yours.