Public Health and the Public
Are Fauci, the CDC, and others getting a bum rap?
Kevin Drum offers “A Brief Timeline of CDC Advice.”
1. Somebody publishes research suggesting that things have changed. This gets reported.
2. A cadre of loud and persistent critics begins demanding that the CDC skip its usual bureaucratic dilly-dallying and change its guidelines now. Science has spoken. This gets reported.
3. Someone leaks the news that the CDC is thinking about announcing a change. This gets reported.
4. The CDC announces new guidance. This gets reported
5. A new pack of critics begins yelling that the CDC blew it and the guidelines really should have stated something different. This gets reported.
6. Someone finds a source in the FDA who says the the CDC never consulted with them, and this explains why they screwed things up. This gets reported.
7. The CDC explains its guidelines with some added nuance. This gets reported.
8. Every doctor and pseudo-doctor on TV, radio, and social media begins to loudly debate the guidelines. In newspapers and on local TV, reporters produce pieces listing the pros and cons of each side.
9. After inhaling all this, half the country complains that the CDC waited too long. The other half complains that they acted too quickly and caved to political expediency. A third half complains that they just can’t keep up with the CDC’s constantly changing advice.
10. Somebody publishes research suggesting that something else has changed. This gets reported.
Rinse and repeat.
Commenter Joel approvingly adds,
The Nobel Laureate economist Paul Samuelson famously acknowledged in a Meet the Press interview: “Well when events change, I change my mind. What do you do?” This observation applies to the advice from medical authorities such as the CDC and WHO during the COVID pandemic. Some members of the public are fond of pillorying these agencies for having published different guidelines at different times, as though health officials are in the business of issuing ex cathedra dogma rather than responding to incomplete and ambiguous information. Science doesn’t deal in proof, it deals with the weight of evidence. A scientific hypothesis is one that is capable of being tested and falsified by experiment.
I get it. I used to teach problem-based learning to first year medical students, and they often struggled with what to do with incomplete and ambiguous information, which is what physicians in clinics do every day. Sometimes, one cannot wait for all the tests to be completed and all the data analyzed before taking some action. With new evidence, a change in action is sometimes warranted.
Thanks to COVID, the curtain on research and discovery has been pulled away and the omniscient Oz is revealed to be a mere mortal doing their best with the resources at hand. So when new and better data appear, it is right and responsible to examine previous advice in light of those data. This happens all the time, even if most people don’t see it.
So rather than prating at the CDC for evolving standards in light of new data as though discovering that papal bull was found to be papal bull****, celebrate the fact that science is self-correcting and, overall, moves towards better understanding. To paraphrase MLK: “the arc of the scientific universe is long, but it bends toward truth.”
And Clawback piles on,
I’m always amazed at the inability of people to deal with uncertainty. Look, it’s a “novel” coronavirus, right? Almost nothing was known about it initially, and it takes time to understand its behavior, especially since it’s constantly changing. Any official advice is going to be preliminary and you’re going to have to use judgment when applying it.
I guess critical thinking just isn’t really a thing among either our elites or the public.
And Salamander takes it a step further:
The public/pundit rage-fests seem a part of the American public’s drift into absolutist, babyish, dogma-based thinking. Look at Bush the Lesser and his endless use of the infantile term “bad guys”. Also, the bible-beater domination of the Republican Party and their reliance on immutable, fixed, scriptural “truth.” Which, incredibly, can change for them daily, based on the current moods of their new dark god — but that’s OK!
The rise of what was once billed as “24 hour news” channels, which in fact amount to 24 hours of every opinionated talking head addressing the same small story — or non-story — over and over and over, all day long, has helped propel these stupidities and rushes to judgment, as has the speed of the several internet gossip “apps.”
If the public was better at critical thinking, evaluating information, detecting bull, the problem wouldn’t be as severe, and lots of companies would have to find other ways to make themselves filthy rich.
There’s clearly a lot of nonsense in the public debate over the CDC guidelines, attributable to many causes. The politicization of the virus by former President Trump and the right-wing infotainment complex hasn’t helped. Republican governors and mayors have followed suit, taking idiotic stances against masking, vaccination, and other measures. Whether in reaction or because of different circumstances, some of their Democratic counterparts have gone too far in the other direction, treating masking and the like as a shibboleth. This has all been compounded by the natural attitudinal and cultural differences between densely-packed urban centers and rural and suburban areas. Add in the American “you can’t tell me what to do” attitude, an Internet that makes everyone think they’re a medical expert because they can “do my own research,” and social media bubbled and algorithms that feed them just for fun.
At the same time, let’s not pretend that the CDC guidelines are simply the evolving scientific consensus on an emergent and constantly evolving situation. As I’ve noted many times as this has unfolded, public health isn’t just about the science, it’s about messaging, incentives, political realities, and balancing competing policy priorities.
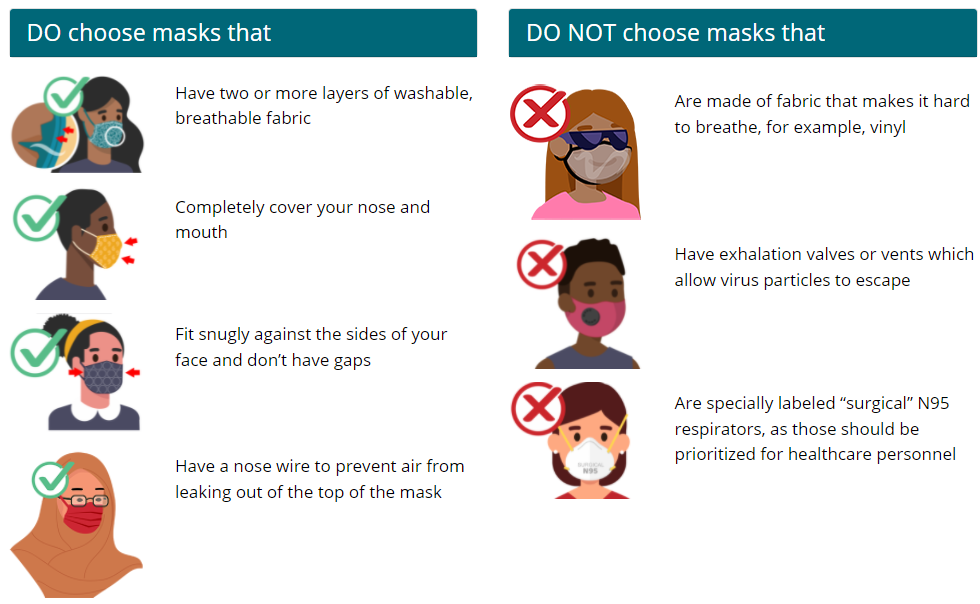
Public health officials deliberately lied to the American public about masking because we had limited stocks of medical-grade respirators and surgical masks and didn’t want panic buying to take them away from frontline workers who needed them more. Way too late, they decided that, well, cloth masks would be okay. And way, way too late they told us that, well, cloth masks aren’t really all that valuable and we should upgrade to medical-grade masks–but preferably the ones from Korea rather than the ones American healthcare workers use. This, not unreasonably, sowed confusion and distrust.
Similarly, when they issued guidance that fully-vaccinated people should be allowed to go about their lives (with modest exceptions like masking on airplanes) just as they did before, they were making a public policy choice, not a medical one. They reasoned, correctly, that this would encourage people to get vaccinated, which was the best way to get to “herd immunity.” But, because the politics mitigated against vaccine passports outside maybe a handful of tightly-packed cities, this also allowed the unvaccinated to free ride and almost certainly contributed to the spread of the virus.
CDC director Rochelle Walensky has admitted that the agency has done a bad job of communicating with the public. Part of it is simply a function of trying to distill a complicated decision tree into simple recommendations. Part of it is genuine disagreement among the top researchers in the field as to what the evidence shows. Part of it is balancing competing priorities.
So, absolutely, too much of the criticism of the CDC is just a function of non-experts watching the sausage being made and not understanding or liking what they’re seeing. But a lot of it is the fault of officials doing a bad job of the public part of public health.



The CDC’s problems have not merely been those of communication and evolving knowledge. Unmentioned in the above is how the CDC bungled the development of COVID-19 testing early in the pandemic.
I think we need to review how our healthcare bureaucracies function not limited to the CDC but extending to the FDA as well. But now is not the time for that. I’m not among those who think that we should rely solely on the private sector but I do think that we could and should improve how our bureaucracies function.
@David J Schuler:
You’re right, but I suspect that you know as well as I why bureaucracies in general, both public and private, stumble along, inefficiently addressing issues that are no longer the burning problem.
Today the major public health communities of interest, drug companies, medical providers etc, are pretty happy with how the CDC and FDA function, they know what buttons to push to get what they want. The dissatisfaction is coming from emerging communities that don’t see their concerns begin addressed. To make matters worse, to truly realign the CDC and FDA will require congressional action (even more so with this Supreme Court), and we know just how vigorous a legislative machine our Congress is.
@Sleeping Dog:
I agree that “regulatory capture” is a major issue. It’s one of the factors that would need to be addressed in the review I imagine. And thank you for mentioning that private bureaucracies present problems as well. I couldn’t agree more.
Losing track of their notional mandates is inherent in bureaucracies. We’ve known that for more than a century, since Max Weber pointed it out.
CDC has displayed all the signs of an aging organization filled with entrenched bureaucrats who cannot pivot from the status quo.
When an organization reaches this level of maturity they hadle familiar challenges quite well. The flip side is they soil themselves royally in an emerging crisis. Its is very important to maintain a balanced of experience and youth in an organization because most of your revolution ideas and unconventional thinking is going to come from the younger members.
Just a guess but Id be shocked if the CDC wasnt extremely heavy in people 5-10 years from retirement. Their messaging sucks, their overall campaign approach was flawed from the beginning.
Biden should really focus on reorganizing the CDC so its better prepared to deal with a follow on crisis in the next 15-20 years. We can’t afford for them to fail again.
As Everlast pointed out, You know where it ends, yo, it usually depends on where you start.. Good or bad compared to what?
I’ve realized, engaging as I frequently do with my angrily idealistic oldest daughter, that she judges actions by contrasting what is against a model of perfection. Being an old man I contrast what is against what experience has taught me to expect, which generally, is bumbling, confusion, stupidity and cupidity. If you expect perfection you will be disappointed every single time, which is appropriate I suppose for the yutes. The olds are more likely to be amazed any time something isn’t a complete shit show.
By the standards of realistic expectations the CDC has done OK. Not great, but again, an unprecedented, two year-long and counting pandemic is a pretty severe stress test for the system.
Personally I’m just amazed the wheels haven’t come off completely.
Future CDC messaging will have to take into account the now-evident fact that about a third of the population are morons and will need their instructions to be accompanied by brightly-colored stick figure illustrations, perhaps a puppet show and maybe a catchy tune. I suggest reaching out to the producers of Blues Clues and Dora the Explorer.
For some folks it is “Call my Preacher/Rabbi/Cleric so he can tell me what scripture says.”As Salamander pointed out, it is “their reliance on immutable, fixed, scriptural “truth.”” which lets face it, isn’t.
Only the laws of nature are immutable and fixed, and our understanding of them is the barest of minimums.
@Jim Brown 32:
How much of the organizational structure, charters, and procedures are actually in Biden’s control? And how much of it would take Congress acting?
@Michael Reynolds:
And it’s a severe stress test being executed in the glare of a global media spotlight 24/7. That CDC director Walensky still thinks the agency could do better tells you what you need to know about how hard those bureaucrats are trying to get it right the first time.
I think Drum is largely correct, although I agree with James that the CDC is not just processing science and that explains everything.
But I would note that the whole mask debacle, which was a massive mistake, took place early (very early, in fact) in the pandemic. The fact that this is the gold standard story, cited every time anyone talks about this general topic, is telling to me because if the CDC was just an utter disaster, we would have a lot more to criticize than repeating that story over and over as THE example.
It is also hard to separate out what the CDC did right or wrong and what the broader federal government did. “CDC” becomes a container to put all our public health frustrations.
A few thoughts:
1. The Trump administration made it impossible to have a coherent policy on the pandemic from January of 2020 to January of 2021. This is the heart of all of this.
2. The Biden administration utterly over-estimated how many people would get vaccinated, and planned incorrectly.
3. Delta and then Omicron.
@Michael Reynolds:
This is a common intellectual malady–and not just among the young.
I often have to tell colleagues that, obviously better is always better, but what are the odds we can generate better? And perfection is just utterly out of the question.
This tends to be my view as well.
@Steven L. Taylor: I highlight the mask example because it’s the only one that I can think of that was arguably malfeasance: they deliberately misled the public. The biggest case of misfeasance, also very early, was the one @David J Schuler points to: the fiasco over testing combined with a bureaucratic insistence that we wait around for them to get it right rather than pivot to one of the many already-proven options already available. Mostly, I agree with @Michael Reynolds that they did pretty well, all things considered.
And, yes, there’s really no way to know how much better this all would have been had a competent, non-malicious President been in charge in the first year-plus.
From my POV the CDC not only blew the mask issue but also screwed on more important stuff. The testing was big as Dave pointed out and they also hung on to the idea that you cannot have asymptomatic spread well beyond the point when twins obvious it could spread that way. The clearly made some errors.
That said it was a new virus and they had a huge handicap in Trump. After their poor start they did better. I would give them a C+ or B-.
Steve
@James Joyner:
Yes, a thousand times, yes.
@Jim Brown 32:
“Biden should really focus on reorganizing the CDC ….. ”
As opposed to focus on voting rights or democracy, or poverty or infrastructure (hard and soft), domestic terrorism, anarchists, international security, immigration reform, or,…. or …..
Yes, CDC and bureaucracy in general needs to be somewhere on the priority list but I doubt that it’s really in the top 10.
One issue I think the CDC and FDA have had is that they’re sticking to procedures designed for normal situations instead of adapting to the reality of a pandemic.
In particular, regulatory approvals tend to be pretty conservative (in the philosophical sense, not the political sense): it’s better to do nothing than to do something that later turns out to have been a mistake.
The problem is in a pandemic where each additional day of waiting means another thousand people die, there’s a very real cost to doing nothing, and it seems like they’re failing to adjust procedures to account for that.
@Stormy Dragon:
e.g. one specific example was adding a three month delay to the Pfizer EUA for 5-12 year olds to collect additional information when it’s been pointed out the information they wanted to wait for was unlikely to significantly change the results from what they already had.
@James Joyner:
But that’s my point: it is the only example of malfeasance. Yet, in every conversation on this topic it is the example of what is wrong with the CDC’s response.
It reminds me of conversations about concerns about radical Islamic terrorism in Latin America: every story had to cite the Hezbollah-linked bombing in Buenos Aires in the 1990s because it is the only really good example of the alleged problem.
And, yes, we have done a terrible job on testing. I don’t think that is a CDC thing, per se (more an FDA thing, yes?).
Indeed, was the mask thing even CDC-specific? I link it more to Fauci/maybe NIH.
@Bob@Youngstown: @Bob@Youngstown: Indeed and indeed.
@Steven L. Taylor: Yes, testing was definitely the CDC. NPR from November 2020: ” Early in the pandemic in February, a test designed by the Centers for Disease Control did not work, which setback U.S. efforts. Now, an internal investigation from the CDC obtained by NPR shows the microbiologist who produced that test knew it was flawed and sent it to the nation’s labs anyway.” It set us back months.
And, yes, while Fauci was the most visible person lying about masks, this was CDC February 27, 2020: “CDC does not currently recommend the use of facemasks to help prevent novel #coronavirus. Take everyday preventive actions, like staying home when you are sick and washing hands with soap and water, to help slow the spread of respiratory illness. “
@Stormy Dragon: I take the point, but one can also argue that being liberal with approvals (in the manner in which you are using the terms) can also lead to very bad outcomes, especially in an emergency.
I am not going to defend any specific action, because I have no real basis, but I think a lot of criticism in this falls into the category of what MR was discussed above: assuming that whatever the FDA did was worse than some imaged outcome. This is not at all necessarily the case.
In other words, it seems to always be the case that when (and not just in this context) the FDA is criticized for being slow, the assumption is always that if they were faster, only good outcomes would flow from that. But that cannot be assumed to be true.
What if they rushed tests that ended up being faulty and then this results in more asymptomatic people going out into public and infecting others?
@David J Schuler:
I need to revisit the Weber essay, but I don’t remember that part of his argument (unless you are referring to the shift they make to preserving the bureaucracy itself). What a good excuse to reread that essay.
Beyond that, I’m more sympathetic to the CDC’s situation largely because what they’ve had to do for the last two years is not something they are optimized for. Getting back to Weber, the value of a bureaucracy is in the stability and protection its systems provide under most circumstances.
The problem is that we haven’t been living through “most circumstances” for the past two years.
The challenge we face, or rather the folks in the CDC face, is how to structure themselves so they can effectively deal with the mundane events that they typically deal with AND be better structured for (hopefully) once-a-generation (if not a century) global pandemics like the one we are living through.
However, I’m not sure you can optimize for both at the same time effectively in the same organization.
Regarding testing, the Seattle Flu Study, funded by the Gates Foundation, was doing widespread testing in early 2020 to determine how quickly flu was spread, and discovered an individual with flu-like symptoms who didn’t have the flu. They tested them for SARS-COV-2 and it came back positive. This was how it was discovered that community spread was occurring, rather than people bringing COVID in from overseas. This is what followed:
Link
@Stormy Dragon:
Yes to both of your posts. The morality of inaction (delayed action) is often ignored in these defenses of the agencies. Messaging malfeasance – real as it may be – is arguably of lesser consequence.
On the other side, many of the critics (especially the more obnoxious ones) fail to appreciate the differences amongst CDC, FDA, NIH, etc. And don’t get me started on the lack of statistical fluency.
@David J Schuler: @Jim Brown 32: @Michael Reynolds: What Reynolds said.
But I’d go even farther: I think the CDC response has been pretty darn good, with two exceptions (I’ll get to those in a subsequent post), and considering the avalanche of sh*t that rained down on us all, two exceptions is a pretty good track record. Mostly it is a problem of the public’s expectations. They think the CDC is something that it is not, and judge it harshly because it isn’t doing things that it has no legal right to do.
The CDC is not our National Health Agency. They have no hospitals, do no laboratory research on their own, don’t administer vaccines or medicine, they can’t shut down or sanction bad actors, in fact, they have NO authority to make anyone do anything. They are an organization whose purpose is PUBLIC HEALTH. They determine the top causes of poor public health, analyze the research on both the medical (where that is relevant) and social (always relevant), develop best practices, issue summaries of the above to the general public (which is unread by 99% of the public unless it concerns things related to sex or guns, and then they are only reading it to get angry). They also (and this is the bulk of what they do) coordinate with local and state health departments, as well as the health agencies of other nations to disseminate those findings and collect new data.
Aside from the military, the US does not have a National Health Agency. Full Stop. We really on private businesses for our health. We do regulate their actions (the FDA) and provide guidance (the CDC). Expecting the FDA and the CDC to become the National Health Service in a crisis is merely blame shifting. We, as a country, have decided we don’t want a National Health Agency. The blame is on us as a country. To give you an idea of the effectiveness in vaccination policy in a country with as many wackos and a clowns as the US but with a National Health Agency, look at how Great Britain is doing. Nearly 90% of those over 7o have been fully vaccinated AND boosted!
@Steven L. Taylor: @Stormy Dragon:
The word Thalidomide still sends shudders up the spines of people of a certain age. My parents had a friend with a Thalidomide baby. Let’s not be too quick to pull the trigger on approvals – a serious issue with the vaccines would have doomed public health efforts and we’d all fucking die of Covid.
@James Joyner:
I took that at the time to be a white lie intended to avoid a run on PPE which were in very short supply.
@Michael Reynolds:
I was thinking Thalidomide too. That said, that was more of an FDA issue than a CDC–though both are interrelated. Honestly, I don’t think I can easily articulate off the top of my head specifically what the CDC mandate is–beyond “controlling disease” of course. And my understanding is that “disease” in this case is a pretty wide category of ailments and afflictions.
@Steven L. Taylor:
Hmmm…my experience has been different. The people I’ve been reading on this (specifically, from the critics camp) have been rather good on grappling with the probabilities. And the unknowns. Hell, many of them are avowed Bayesians! I may not always agree with them, but I don’t consider them to be painting overly rosy counterfactuals.
@Michael Reynolds: As noted in the OP, I agree that’s why the public health leadership lied to us. But it naturally led to distrust.
@James Joyner:
Today, it is accepted wisdom that masks work. There is some small evidence for that. Not a lot, and it’s not very robust but, two years into this, we do have a little evidence. At the time that statement was issued, however, there was no evidence. Zero. In fact the one well done study, which was done in Indonesia after (during?) SARS, showed that encouraging surgical mask wearing by family members caring for or living with a sick person were slightly, very slightly, less likely to get sick themselves.
James, it sucks that we didn’t know then, and don’t really know now, whether and how much wearing masks reduce the spread of disease. As you know, my company’s equipment is used to test filtration material, masks and cartridges, so it would be great for our business if we promote studies showing how effective N95 mask wearing by the general public is in preventing COVID. There is no such slam-dunk evidence.
Fauci wasn’t lying, the CDC wasn’t lying. Given what they knew then, that a) surgical and N95 mask wearing as part of a complete protocol including face shields, gowning, sterilization of equipment, constant cleaning of surfaces, gloves, enforced hand washing, etc, has been proven over the course of decades to dramatically slow the transmission of disease in health care facilities that can enforce these protocols with the threat of termination, and b) that encouraging family members of sick individuals to wear surgical masks whenever they were around them had a very moderate positive effect in a single experiment (and it was entirely reasonable to assume that this modest improvement would fall away for motivating mask wearing around healthy individuals).
It wasn’t a lie. Given what we knew, there was no reason to believe that encouraging widespread mask wearing was going to do the general public any good, and it was definitely going to worsen the shortage for medical professionals, so they recommended against it. I believe they made the right call.
One more thing on masks: We confuse the individual health aspects of mask wearing with the public health aspects.
The individual: if I regularly wear a cloth mask, will I reduce my likelihood of contracting COVID (assuming that, aside from the mask, I take all other precautions equally)? What about a surgical mask? What about an N95? What about a P100 respirator, properly fitted? Before we can assess those things, the answers to the following questions are important: Is the virus mostly transmitted by contact or is it airborne? If it is airborne, is it considered a particle, which drops to the ground in roughly two meters, or an aerosol, which can hang in the air for days? If it is a particle, are they big, like droplets, and so could be stopped by a tight cloth mask? Or are they tiny, smaller than dust but larger than an aerosol, that won’t even notice a cloth mask? For the individual, especially given that we didn’t know any answers at the beginning of the pandemic, if you can wear a mask it is unlikely to do harm, and might do good. The more filtration in the mask and the better it fits, the better. For me, I settled on an N95 as the maximum I would wear every time I was in public, absent conclusive proof that it was worthless.
Public Health: Absent these answers, is the best use of a public health organization’s finite time, resources and credibility promoting mask wearing in the general public?
I honestly think the answers in both cases are pretty clear.
@Michael Reynolds:
@Matt Bernius:
That was kind of the point with my specific example: if they were actually concerned about some thereunto unknown issue, the additional trial would have had to have been far larger than it was. As it is, they delayed three months collecting data that would have been statistically unlikely to detect anything that hadn’t already been detected in the original trial.
If their concerns were of a “thalidomide” situation, then their response was purely a CYA gesture.
That’s exactly what it was, and I’m still not sure where I fall on this. It was dumb to lie, because it nonsensical on its face–of course masks work. Medical professionals don’t wear them because they look cool with the outfit.
If we had an altruistic public, the truth might have worked, but we all know that most people are going to act in their own self interest first. The truth would have caused an outright run on supplies, leaving already vulnerable medical professionals at higher risk. Remember, early on, the deaths of health care workers was very high.
None of this matters anyway. We’ve learned in the interim that a certain percentage of people don’t GAF about what professionals/experts say. They’d rather listen to their holistic health healer or chiropractor or preacher. /shrug emoji
@Matt Bernius:
Controlling disease from a center. Don’t forget the center.
Why don’t we separate food and drug? Hamburger and mRNA are not really the same sort of thing.
@Jen:
See my posts above. There is no “of course”. I religiously wear my mask whenever I’m in an enclosed public space, but there is little robust evidence that masking, as a public health policy, works. And what little exists came after those initial statements. I wear it because I know an N95 mask can filter out the virus, and that there is evidence that reducing the amount of the virus you are exposed to lessens the impact to your health if you get sick. I haven’t worn a cloth mask since the early days.
That sounds like a slam for some reason [eyeroll]. I’ll just go on record that Korea offered the best medical care that I had gotten in my adult lifetime and that Korean manufactured pharmaceuticals and medical supplies seem pretty top notch to this little bunny who used them for most of the previous decade.
And Seoul had a really bad breakthrough last week, according to a friend who lives there. About 50 or 60 new cases–in a city of roughly 10 million. My county, population 110,000, had 174 new cases last week along with 46 (IIRC) ‘unconfirmed cases.’ Having some Kf94 masks here would probably be a good idea. I know I’ve ordered a box.
@Jim Brown 32: “Biden should really focus on reorganizing the CDC so its better prepared to deal with a follow on crisis in the next 15-20 years.”
Yeah. The next (GQP) Congress will be right behind him on that one. They’ll be the ones trying to push him off the cliff.
@James Joyner: “@Steven L. Taylor: I highlight the mask example because it’s the only one…” [emphasis added]
Which is EXACTLY Dr. Taylor’s point.
@Just nutha ignint cracker: Technicalities aside, the Korean masks meet the same standards as the N95, except for the 94% vs 95%, which is not significant.
@Michael Reynolds: Also a firm belief that masking was relatively unimportant (IIRC, the conventional wisdom at the time was that Covid-19 was more like the common cold than pneumonic plague or Tuberculosis as was more likely to be caught shaking hands with someone than being sneezed on (or breathing the same air as an infected person in close quarters). Beyond that it took Asians to figure out how to make a handkerchief and a couple of scrunchies into a pleated mask that covered the whole face. (I had some really nice–and large–silk or rayon handkerchiefs that made 4 layers of covering over my mouth when I folded the ends into the center. I hope that Dr. Fauci was failing to make these suggestions because he didn’t know them. We’re really lacking in makeshift masking technology outside of the criminal element here, as you well know.)
In the above quotes there are a couple of gems in terms of how to think and talk about politics.
From Clawback,
Indeed. Most people see the world in black or white, they don’t do well with gray. It’s part of what Reynolds used to talk about as a lack of imagination. A trivial but common example – how often have you turned into a grocery store aisle and found someone with a cart crosswise blocking the aisle. They invariably politely apologize and move the cart. But did it not occur to them that someone else might push a cart up a SUPERMARKET AISLE? It’s an inability to see beyond what’s immediately apparent. Is COVID transmitted by surface contact or airborne? Well it’s one or the other, why won’t you tell us which?
Salamander says,
Which, incredibly, can change for them daily, based on the current moods of their new dark god — but that’s OK!” It’s more than the holy rollers, it’s conservatives. Like the meme says, conservatism is opposition to what liberals are for today, updated daily. Deficits are OK if Moscow Mitch is Majority Leader, evil if Schumer is. As Clawback says, they aren’t good with uncertainty, but they’re fine with contradiction. 1/6 was Antifa terrorism, it was FBI entrapment, they were harmless tourists, of course they responded when TFG told them to fight, TFG had nothing to do with it, and on and on. It’s nailing jello to a wall. Fixed principles of conservatism is a category error. It’s all revealed faith. They believe what they’ve always believed. And tomorrow they’ll have always believed the opposite.
I’ll add one of my own,
Did the CDC do everything right? No. Were they evil? No. Is there room for improvement? Yes. Did they get things mostly right? About as close as could be expected, all things considered: “novel” coronavirus, shortages, hostile top leadership, public resistance, media laziness and ignorance. Is it helpful to kibitz everything they do? No.
@MarkedMan: The aerosol question wasn’t considered early enough — apparently, western medical specialists just don’t believe aerosols are common or something, and that it must be spread via droplets so the virus in kept nice and wet.
(Western meaning European and American, not meaning “as opposed to folk medicine” — for whatever reasons, the medical establishment in Asia looks at the same inconclusive data and says “we haven’t shown that it is merely in droplets, so we should assume aerosol”)
(Reporting has been weird on this — including an article in Wired of all places — so I may be getting parts of it wrong)
IMO Drum elides the actual problem that people are complaining about, which James touched on. Reasonable people understand that science changes and circumstances change which affects recommendations. That is not the issue.
The issue is the CDC has violated their own communication guidance at every turn, they continue to make decisions and recommendations based on factors other than science in an untransparent way, including outright deception.
This is in addition to the CDC’s continuing failures of its core competencies. Drum and the others elide all this with their strawman that people just can’t handle changing science. When the reality is the opposite – the CDC has been, in many instances, way too slow to change its recommendations.
@Michael Reynolds:
I have no idea whether this is sarcasm or not, because it is pretty much spot on with what needs to happen.
Who will ever forget “if it’s brown, flush it down; if it’s yellow, let it mellow”? Certainly not the Donovan estate, as the song Mellow Yellow will forever be linked with urine.
On the other hand, how many people actually understand how a bill becomes a law or what a conjunction is?
And no amount of clever rhyme will help if people are actively opposed to Conjunction Junction and think it’s part of a plot to mandate compound sentences and change the English language so we are all speaking Chinese. (German would probably be a better example, but many of the people who would object actually really want to speak German…)
@Michael Cain:
There is a lot Biden could do. For one, tell the CDC to stop the noble lies and get them to be transparent about their recommendations. We shouldn’t have to read the back story in the NYT or WAPO investigative reporting to discover that some recommendations are made for political reasons. The administration should be doing the political balancing, not the CDC.
@Michael Reynolds:
True, there was a shortage of PPE. However when dealing with a crisis from a position of leadership it’s usually best to play the long game. Once credibility is lost it’s difficult to all but impossible to get it back. Full disclosure is the way to go. They should have trusted us.
@Just nutha ignint cracker:
This was one of the two mistakes of the CDC that I alluded to in my first comment above, and it should be a much bigger deal. However, it’s hard to blame the CDC for it, since it was actually a mistake that virologists have been propagating for a half century. Bottom line, an influential virology paper way back in the mid-twentieth century stated that any particle smaller than 5 microns is an aerosol and will remain suspended, while anything larger than that is a particle and will drop out of the air fairly quickly. (The COVID virus is 100 microns.) This was simply a mistake by the author, but the paper was influential and scientists rarely step out of their domain. In reality, the dividing line is at a 1000 times that size. I just looked up settling times and the measurement for the smallest particles I could find was 500 microns (100 times the size stated in the paper and 5 times the size of a COVID virus) and that was 41 hours. In fact, the aerosols we generate are centered around roughly 200 microns, and those are considered pure aerosols by the industry. All of this was known when that paper was written.
This is the big scandal. This mistake is why the CDC and everyone else thought masks wouldn’t make that much of a difference, at least as compared to social distancing. If the particles hit the ground in 5 feet (the standard belief amongst virologists) then spending your effort on getting people to stand 6 feet apart gives the most bang for the buck. And this mistake didn’t just impact COVID response. It has influenced the way we react to disease spread for decades. It wasn’t until COVID that people other than virologists were reading CDC warnings and other explainers. I often rage against the “random guy on the internet outthinks the experts because they are a bunch of sloppy dummies”, but this time it’s true. Or, at least, “random environmental aerosol specialist outthinks the virologists on this one crucial thing.”
@Andy: Have you ever read any CDC guidance? It’s all there on their website and, if you dig down a few layers, how they came up with it, everything they took into account, etc. I would guess that, like most of us (and that includes me, 95% of the time), we read the press coverage of the announcements, which include none of that. Hell, because of what I do for a living, I go maybe one level deep into the research on masking, and even at that level it’s an incomplete jumble.
When the CDC crafts a message for the general public, it must be very short, and very specific. A couple of centuries of experience shows that to be the only method that has a chance of affecting public behavior in a significant way. The CDC does a lot of work to craft that message and, in fact, it shows that work, but it does so separately from that concise message. It seems to me that what you describe as “lack of transparency” is really, “I want a message that is no more than two sentences long but then contains all the thousands of considerations that went into that message.” You want the background, it’s on their website. You want someone to distill that background into the best short, actionable advice? That’s what those press releases are.
@Just nutha ignint cracker and @MarkedMan: South Korea is a fully modern country and a longstanding ally. It’s just rather amusing to me that they push the Korean knockoff of the N95—which, by the way, is what I’m currently using—rather than the N95 itself.
@Just nutha ignint cracker: Steven and I agree that the CDC is run by professionals who are actually trying to get us through this damn thing. I highlight the one egregious, early example of malfeasance because it, quite naturally, helped create distrust.
@MarkedMan: Fauci himself has all but admitted that his primary concern (and, that of the CDC and other public health decisionmakers) was preventing a run on PPE needed for healthcare workers. I’m sure that we know more about the effectiveness of masks now than we did two years ago. But it was commonsensical that wearing masks was more effective than not against a respiratory ailment.
@Steven L. Taylor:
Except it isn’t the only example of malfeasance. It’s just the best-remembered and most obvious example because it was such a bald-faced lie, and because they later admitted it was a lie. And, like many things in life, first impressions matter and are what people remember most.
Consider the CDC’s recent change in quarantine guidance from 10 to 5 days with no testing required. Many experts were puzzled by this on a scientific basis, but then the NYT and others reported that two major factors in the decision to change the recommendation were concern that a 10-day quarantine would shut down too much of the health system and economy, and that the choice not to recommend a negative test at the end of 5 days was driven by the fact that, unlike every other major industrialized nation, the US still has a test shortage. They couldn’t recommend testing because there still isn’t enough testing capacity. Although the CDC, in response to criticism on this, now says it may revise that – so get ready for another flip-flop.
Now, both of those are valid reasons for the guidance they gave. Given the choice between, for example, hospitals, critical business, and schools shutting down because 10-day quarantines from Omicron would gut staffing, and taking on more risk and increasing Omicron spread with a 5-day quarantine with no testing, the latter is, I think the right choice. The problem is that they weren’t transparent about those reasons and instead kept insisting it was all about the science.
Or another big one was FOIA release showing that teacher’s unions influenced the crafting CDC school reopening guidelines including adopting some of the union’s suggested language.
Now, getting input on changes from interested parties is fine – as long as you disclose that’s what you’re doing. But don’t claim that you’re “following the science” if you’re letting some stakeholders see and influence your proposed guidance before the public sees it.
Those are political tradeoffs the CDC should at least be disclosing. But ideally, they shouldn’t be doing that at all. That’s not part of their job. The CDC should be providing information, coordination, research, etc. It should operate like the intelligence community – informing policymakers who then make decisions and implement policy. But what has happened is that policymakers don’t want to do that – so it gets pawned off on the CDC which then tries to sell the recommendations as “science” when it’s clear it’s not just about science or the optimal strategy for fighting the pandemic.
@MarkedMan:
But this is how they got in trouble on the PR front. When they are simply taking their best educated guess they need to be transparent and explain it in depth in order to maintain credibility. Treat people as adults and they might act like adults, treat them as children…
Somehow the italics got transferred from the quoted to my comment in the above post.
@James Joyner:
I don’t think it’s fair to call it a knockoff. The masks are denoted by the standard to which they are tested and that’s dependent on the country they are sold in. If you sell in the US it’s the NIOSH N95 (95% or better) standard and so we call them N95 masks. In Europe you can only sell FFP2 (94% or better). The Koreans use KMOEL (94%) and the Chinese use KN95 (95%). Here’s a handy chart. Considering that the Europeans and the US have spent more than a half century harmonizing standards and still aren’t there for masks, it’s hardly surprising that other countries have their own standards. (Not useful, but not surprising.)
@Gustopher: I suspect that part of the problem is that Western peoples may, in general, less disposed to the notion that no one is wrong 100% of the time. I bring up the question because of the concept in the ancient and mediaeval worlds of the idea of diseases being caused by miasma–bad air being trapped in an area. As I understand (in my grossly oversimplified manner) the pseudo folk wisdoms that accompany this topic, the discovery of germ theory discredited the idea of miasma to an impressive degree. So impressive, in fact, that we decided to pretty much abandon the notion of miasma. Leaving us vulnerable to an array of immerging aerosols that make the air bad.
In fairness, we haven’t seen–or paid attention to, not sure which–aerosols as sources of infection for quite a while, so maybe this disconnect would have happened anyway. It’s just interesting to me that miasma, a discredited idea from the primitive ancients, seems to be making a comeback in a spiffy new outfit. (very chic!)
@dazedandconfused:
That’s the point – they do explain it in depth. It’s just that the news media doesn’t report on that. But you can find it if you dig around on their website. Early in COVID my wife had a gig with a team centralizing all the recommendations, analysis and research from the main health agencies around the world and distilling it for an International NGO’s clients, who were almost always professionals and usually health professionals. For every 2 sentence recommendation from the CDC they have a 2 paragraph one with more detail, a 2 page one with still more detail and then a whole slew of analysis those are based on (the 2/2/2 is not a policy, I’m just trying to give a feel for it). It’s all there. But no one looks for it. No one but public health officials read it. It’s why they work so hard to craft that two sentence message – they know that’s the only thing 99.9% of the population is ever going to come across.
Look at the way this thread is going – everyone is saying they failed because they didn’t provide something that they, in fact, did provide. Even amongst this very well connected group, who all spend way to much time googling all manner of things, we are ready to bitch but never raise a finger to keyboard to actually check whether it was there or not.
@MarkedMan: For me, Dr. Joyner’s comments on the topic continually resonate a message, perhaps unintentional as I have no idea how obtusely spoken he is outside this forum, that “foreign made/classified/whatever” is equivalent to “inferior.” It reminds me of my mom’s question when I left to teach in Korea: “Do they have doctors there? How will you manage your health problems?” Her excuse was that she was 80 and suffering from Alzheimer’s.
@James Joyner: I think it’s instructive to look at another piece of advice they made at the same time: hand sanitizers and hand washing. There was also an instant shortage of hand sanitizer and that made it difficult for medical professionals to get it to. However, the evidence for hand sanitizing through gels or soap is clear and mature and there is good evidence that increased hand washing in the general public would slow the transmission of a virus or other pathogen if it was transmitted via touch. Based on that the CDC made the recommendation, even knowing it would hurt the hospitals to some extent.
In the event, it was the “wrong” call, because it turns out this particular virus isn’t primarily transmitted through contact. But it was the “right” call at the time. The evidence showed that a public campaign of hand sanitation could have been instrumental in slowing down the disease.
Your entire critique of Fauci and the CDC is based on your belief that the CDC believed that a public campaign of mask wearing would have made a significant difference. But the CDC did not believe that, nor did most public health professionals. The limited research showed very little benefit even when public health officials were showing up at peoples door and reminding them to wear the masks. And they (tragically, erroneously) believed that COVID could not be aerosolized based on a half century of mistaken science. They therefore recommended that there not be a public campaign of mask wearing.
So, when they had science that backed them up, they were willing to recommend hand sanitizers even knowing it would cause a shortage. But when they had no scientific evidence mask wearing would work, they recommended against it, knowing it would disrupt hospitals.
@Just nutha ignint cracker: I hear you. I used to believe that buying brand names was a ripoff, and then I spent 20 years or so installing systems in manufacturing plants. Suffice it to say that after seeing a tidal wave of roaches pour out of a piece of equipment*, I will never buy RC Cola or Sam’s Club soda ever again.
*In truth, it was by proxy. I was on the phone with my technician at the plant when he lifted the lid. Let’s just say he made interesting noises.
@Andy: “And, like many things in life, first impressions matter and are what people remember most.”
Or it’s a convenient weapon when the attacker can’t find anything better. It’s like reading right-wingers who hate the fact that poor people have medical insurance. What’s the big complaint about how terrible Obamacare is? That they botched the roll-out of the website and it took a couple of weeks to fix ten years ago. Does that have any effect on how the program works today? Of course not, but it was a mistake and it’s all they’ve got.
I get the same feeling whenever anyone attacking the CDC brings up that hideous lie about masks. Yes, it was wrong. It was also two years ago. Saying “first impressions matter” is basically admitting you’re looking for reasons to hate the government and can’t find anything more recent.
@Andy: ” the latter is, I think the right choice. The problem is that they weren’t transparent about those reasons and instead kept insisting it was all about the science.”
So they’re doing the right things, but in the wrong way.
It’s like the person pulling you out of a burning building who doesn’t stop to introduce himself first. The rescue doesn’t count if he didn’t follow your chosen protocol.
@wr: The interesting thing to me about the CDC mask message was that I read it with the understanding that the main thing they were doing mostly was trying to avoid a run on a market where there was a limited supply. Then again, I’ve spent 25 or so years teaching students that one of the problems that their work will have over and over is that “what you heard/read was not what I meant,” so I may have been putting additional meaning into the statement that others were not adding.
But yes, I thought that the more honest thing would have been to say “we don’t know how much masking will help you, so please save what few masks there are for health specialists and hospital workers in ERs and ICUs.” Also a “but,” no I don’t think that would have dissuaded anyone I know not named “cracker” or “luddite,” so there you are. What to choose…
I’m not that upset about what the CDC told us because a sizeable percentage of America is too stupid to appreciate nuance and too selfish to realise that maybe it’s more effective overall to allow the health service providers to get the damn masks first.
Given the number of Americans who refuse to get vaccinated even though vaccinations would be better for the good of the society surrounding them, can you really say the CDC made an erroneous decision?
@Just nutha ignint cracker:
You’re picking nits here. What they said was “we don’t have any evidence that masking will help the general public, so please save what few masks there are for health specialists and hospital workers in ERs and ICUs.” And that was a true statement.
MarkedMan- I am a compulsive reader and when it has been important to me you are correct that Have largely been able to find good explanations for what CDC does. I agree it is hard to simplify. Still, I would say that they were wrong on more than the masks. Also the testing as was pointed out and they waited way too long to agree that there is asymptomatic spread. Those were very large mistakes. After that they have mostly been OK.
I do disagree with you a bit on masks though you are correct on that one big error that people believed for years. There have been lots of studies on masks before covid. Taken as a whole I think they show that masks do reduce spread. Not a huge effect (not counting N-95s) but enough to be a help. ( I also had to spend a lot of time re-reading on PAPRs. Mom too that literature is actually industrial. Was really hard to find a way to compare N 95s to PAPRs.)
Steve
@MarkedMan:
Re the “we don’t have any evidence” refrain, there’s been quite a lot of discussion about what this means, for whom, etc.
@steve:
I’d be really interested in seeing links to those studies, if you still have them.
@Mimai:There may just be a fundamental difference in the way we look at this. Quoting from the article:
To me this sense of “no evidence” is in no way nitpicky. In fact, it is central to being honest with the public. And the example it gives, about COVID being airborne, is the worst possible example. Saying that there was “No evidence” it was airborne wasn’t a case of being too cute by half, which is what the article implies, it was a cautious statement meant to not overstate what was the widespread belief amongst virologists at the time: that the virus was too big to be airborne. The fact that this was a mistake, the virological community accepted that mistake, and the mistake lasted for a half century is a f*cking big deal, and it is something we can and should investigate and use to interrogate other research. But the CDC didn’t know about that mistake at the time. They were simply, and cautiously, reporting what was the “common knowledge” of the virologist community at the time, but allowing for the fact that some legitimate scientists were questioning that.
Look, I know I’m fighting uphill here. It’s become an accepted fact that the CDC “lied” or “blew it” on masking and whether the virus was airborne. But the fact that it is now common wisdom doesn’t make it true. In both those cases the CDC made the best call they could with the data they had at the time. New data has come in, and the CDC adjusted to that.
@Andy:
I recall an interview with Dr. Fauci about a day after the announcement of the five day window, on the Rachel Maddow show, where he explicitly stated that both the need to keep critical services staffed, and the availability of the sting factored in.
And he also said that the 10 day window was discouraging people from even getting tested, so the expectation was that the five day window, when people are most contagious, plus masking for another 5 days, would reduce spread more than the 10 day window once you factor in compliance.
If you’re not hearing these things, you’re either listening to the wrong sources, or you’re doing a bad job of listening.
@MarkedMan:
It’s not a fight with me. Wisdom is often common and inaccurate.
I’m less interested in tallying the score per se than in understanding how public health officials and agencies manage knowns and unknowns when making assessments and communicating them. It seems to me that, collectively, they’ve been conservative and risk-averse. And this is regardless of who is president.
Don’t get me wrong, I’m all for being conservative and risk-averse. When the situation calls for it. I think there’s a reasonable argument to be made that this wasn’t one of those situations. Or perhaps more nuanced, it wasn’t consistently so.
@MarkedMan: As I didn’t read the larger statement, only the 2 sentences covered by the national press, I missed the detail you just pointed out. My bad. 😉
@Andy:
I’m so pleased that the CDC has won your approval on this issue. They have been waiting to hear from you. /s/
@MarkedMan:
I think that you would find a wealth of information on the basis for testing masks at ASTM F-2100. This standard method (and the justification for establishing mask testing protocols has been in existence since at least 2011.
Unfortunately, as I am no longer an ASTM member, I can not retrieve the background materials (references). But I’d be willing to wager that your employer (in medical devices) would have access. As a former technical committee member, I feel confident that the process of developing a industry consensus standard like F-2100 involved many studies and many hours of discussion and debate.
@Bob@Youngstown: Bob, for the last couple of years I’ve been out of medical devices and instead have been working with a company that makes equipment used to test filters of various kinds, including N95 masks, so I’m aware of the standards used to test those masks. The test protocols are done with a perfect seal around the edges, so 95% efficiency doesn’t represent real world performance. More importantly, a public mask wearing campaign must take into account many other issues. How many people comply, how much of the transmission is via airborne particles versus skin or mucous membrane contact, and on and on. So there is a big difference between the benefits of mask wearing to an individual who rigorously follows protocol and the public health benefit of a concerted mask wearing campaign. At the time the CDC was crafting its advice (and I think still) there hadn’t been much work done in that area, but the little that had been done seemed to show that even with personalized training and reminders from public health officials, a mask wearing campaign was only very slightly effective in stopping flu transmission. Given that the consensus belief amongst virologists at the time was that COVID was not airborne, they made a justifiable call given the information they had.
@Just nutha ignint cracker:
I’m not sure that I’ve commented on the issue before, to be honest. The line in the OP was just an expression of amusement at the mixed messaging. As noted, I’ve bought K94 masks for the family and have been wearing them pretty much exclusively for the last three weeks or so.
As a more general matter, there’s a wide disparity in foreign-made goods. All of the vehicles my family drives are foreign-made. Between us, we have 3 Mazdas, a BMW, and a Nissan. I haven’t owned an American-brand car (a Ford Contour SVT) in 15 years or so, although I believe the Toyota minivan and a couple of the other vehicles were made or assembled in US factories despite Japanese badging.
Most of my dress shoes are Italian or Spanish but most of my casual shoes are probably Chinese-made at this point; the running shoes almost certainly are.
Indeed, the only foreign country I consistently associate with poor quality is the PRC. I buy a lot of their stuff despite that, simply because it’s so cheap and ubiquitous (especially on Amazon, where it’s usually hard to figure out the country of origin before purchase). But they have demonstrated time and again a willingness to flout international standards so have earned a reputation for shoddy quality. Indeed, returning to the initial subject, the Chinese-made N95 knockoffs are notoriously bad and there have been multiple warnings from government agencies to avoid them.
@MarkedMan:
These test standards were not intended, nor do they purport to be representative of “real world performance”. Generally these standards are intended to establish material performance standards under tightly controlled conditions. It is near impossible to replicate the infinite number of conditions that humans deviate from the ideal application, simply because humans seem impelled to oppose using materials according to directions.
I’m sorry if I misunderstood you. Apparently the studies you are seeking are performance in the “wild”, influenced by the wide array of human misuse. Regrettably those studies will almost always have flaws, for humans seem to have an infinite capacity to undermine the intended use.
@wr:
As usual, you are making shit up. I do not “hate the government” (funny considering I worked for the federal government for a 1/4 century) but for whatever reason you seem unable to assume anything other than the worse intentions and characterizations. And you assert I “can’t find anything more recent” yet I gave two specific more recent examples.
I really do not see any purpose in responding to you further since you continue to respond to points I make here in a transparently dishonest way.
@Gustopher:
Here’s the CDC’s press release on the recommendations when they first came out (emphasis added):
That was on December 27th.
It was only after criticism by other experts questioning the weak science justifying t the change that those other reasons came out in later TV interviews as well as a clarification by the CDC which came out on January 4th:
You can google the primary sources for those since OTB doesn’t let me do more than one link.
And this is the problem I’m trying to highlight. The agency only came out with that more accurate justification after it received a ton of criticism from experts along with leaks to the media.
@Just nutha ignint cracker:
The CDC itself states that 60% of KN95’s in the US are counterfeits or fakes. Just because it says it’s a KN95 (or any of the other variants) doesn’t mean it is.