U.S. Death Rate in Drastic Decline
The U.S. death rate dropped drastically last year for the first time since 1938, according to preliminary figures released by the National Center for Health Statistics. This despite a population that is “aging, growing in population and getting fatter.”
Some stats from the AP report:
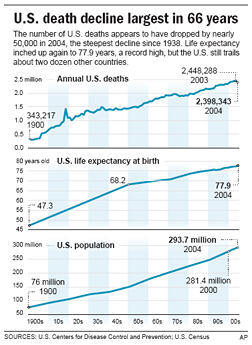
- The government also said that U.S. life expectancy has inched up again to 77.9 years, a record high but still behind that of about two dozen other countries.
Of course, many of those countries do not report data accurately and most of them discount infant mortalities that occur in the first few days.[*]
- The preliminary number of U.S. deaths recorded for 2004 was 2,398,343. That represents a decline of 49,945 from the 2,448,288 recorded in 2003.
- Overall, age-adjusted death rates fell to a record low of 801 deaths per 100,000 population in 2004, down from almost 833 deaths per 100,000 in 2003.
- Heart disease continues to be the leading cause of death, accounting for 27 percent of the nation’s deaths in 2004. Cancer was second, at about 23 percent, and strokes were third, at 6 percent.
- [T]he flu season for 2004 was milder than 2003, which helped explain the more than 7 percent drop in the influenza death rate, Minino noted. The death rates for 11 of the 13 other leading causes of death also declined, with only Alzheimer’s disease (the No. 7 killer) and high blood pressure and kidney disease related to high blood pressure (No. 13) inching up.
- [A]baby born in 2004 could expect to live to nearly 78 — an increase of almost half a year from 2003. Women now have a life expectancy of 80.4, up from 80.1. Male life expectancy is 75.2, up from 74.8.
- [T]he infant mortality rate has dropped to 6.76 deaths per 1,000 births, down from 6.85 the year before. But a huge racial disparity persists. The rate for whites was 5.65 per 1,000 births, for blacks, 13.65.
- The life expectancy for whites — 78.3 — was up only slightly from the previous year. The increase for blacks was larger, with a rise from 72.7 to 73.3.
![]()
![]()
![]()
![]()
![]()
![]()
This, despite President Bush’s well documented hatred of black people?
[*] Update: A commenter reasonably asks for sourcing for this claim. There are likely better cites available but a quick rundown via Google demonstrates the problematic nature of international comparisions, especially between developed and developing states.
The infant mortality rate represents the ratio between deaths of children under one year and the number of live births in a given year. Countries, however, use different definitions for spontaneous abortion, early foetal death and late foetal death (or stillbirth). A stillbirth for example is, generally speaking, the product of a birth that shows no signs of life during and after the whole process of being born. But countries require different lengths of pregnancy to distinguish between early and late foetal deaths (ranging from 21 to 28 weeks). Some countries even require a certain minimum length (varying between 25 and 35 centimetres), some a certain minimum weight (500 or 1000 grams). Differences of definition lead to variations in the measurement of perinatal mortality.
CDC:
Comparison of mortality characteristics of different countries assists health planning and the generation and investigation of epidemiologic hypotheses. International studies, such as studies of the association of aflatoxin and primary liver cancer (4), can reveal a range of exposure levels and disease rates not found in individual countries. However, although death registration is virtually complete in these countries, reporting of cause of death is not uniform either among or within European countries or the United States (5,6). Only comparison of all-cause mortality among developed countries is likely to be accurate. Demographic heterogeneity also constrains the comparison of populations.
Despite worldwide concern, an outstanding problem is how to monitor maternal mortality and to obtain reliable and comparable data. Measuring maternal mortality accurately is notoriously difficult except where there is comprehensive registration of deaths and causes of death. Unfortunately, there are only a few countries where such registration could be characterized as complete [3] and even in these countries, poor attribution of cause of death results in significant underreporting of maternal deaths [4,5]. In addition, countries with complete death registration are countries with low maternal mortality, and, consequently, countries where it is not a public health priority. It is in countries where a reliable vital registration system is not in place where maternal mortality represents a public health problem that cannot be accurately measured.
Several alternative techniques have been developed to fill the gap caused by poorly functioning vital registration systems. Of these, the Reproductive Age Mortality Studies (RAMOS) are considered the gold standard for measuring maternal mortality because it involves identifying and investigating the causes of all deaths of women in reproductive age [6]. Another approach currently used in most developing countries derives estimates of maternal mortality from household surveys or surveys using the sisterhood method [7]. The sisterhood method is an indirect measurement technique that reduces sample size of the surveys by interviewing respondents about the survival of all their sisters [7]. Data on maternal deaths obtained through census has also been proposed as a means of estimating levels of maternal mortality [8]. Drawbacks include high costs in the case of RAMOS, large sample sizes required for household surveys and the use of estimates intrinsically referring to the past instead of the current situation in the case of sisterhood methods. Differentials in the definition of maternal death, varying efforts carried to capture maternal deaths, and the methods used to confirm the deaths as ‘maternal’ are some of the inherent discrepancies in these methods that may affect estimates and impede comparisons. Unfortunately, a measure allowing for comparisons between these methods is lacking.
WHO, jointly with UNICEF and UNFPA, has made efforts to monitor maternal mortality by producing global, regional and national estimates for 1990, 1995 and 2000 [3,9,10]. Different methodologies used to calculate maternal mortality ratios as well as the lack of national data for many of the countries have been identified as major problems in assessing the global situation as well as for monitoring trends. Estimates for 2000 suggested 529,000 maternal deaths worldwide with an average maternal mortality ratio of 400 per 100,000 live births, and accounted for 173 countries with 99% of global births. However, 62 countries (27% of global live births) had no national data available, and maternal mortality estimates for those countries were developed using a regression model based on a set of explanatory country-specific variables that are available for nearly all countries in the world [3]. An alternative model based also on country-specific variables was also proposed using the same data set [11].





All of you kids out there:
TAKE SPECIAL NOTICE
We Old People are going to be around for quite a spell. Better pay attention.
We have the knowledge and the experience to,
Remember US History,
Remember who are and who are not our friends,
Remember who and how we still enjoy the freedoms we have,
Remember who died for us and our nation,
Remember which political party wants to sell our country “down the river”,
Remember who the traitors are,
And, Remember that age and experience are no match for experience and skulduggery
It is not to late for you kids to learn something from we “old timers”.
Well if you’re going to be around can you remember to drive in the right lane?
Only joking.
This cannot be good news for Social Security solvency…
We need more smokers to reverse this trend.
Aw, quit naggin’.
[quietly turns off turn signal that’s been blinking for three miles]
McGehee:
I see you have been following me on the interstate..
You have made my day with laughter. (at myself)
I’ve heard this before but never seen any sources for it.Do you have a cite for this ?
thanks
For once I agree with little shrub, other than the first sentence that should read “all of you neocons out there” and a substitition of the word “wisdom” for “skulduggery.”
*sigh*
I guess we could always hope for mass moonbat suicide…
Don’t do it, LJD. Suicide is not the answer. Seek help now.
I guess being a “little Shrub” and growing rather than being a dead shrub dying like someone we know on OTB that is in dire need for a life.
Ouch! What an embarassing post. Almost makes you feel sorry for little shrub.
Get a LIFE Roger.
Or are you already among the dead?
Must you continually show and demonstrate you total lack of life. The Liberal fertilizer you throw around is beginning to create a smell like that which is thrown around by your Liberal friends.
Ouch! Another embarassing post. Almost makes you feel sorry for little shrub even more, if that were possible.