What’s Wrong with this Picture?
We spend more per capita than any other country in the world and yet we are outperformed on a key metric, life expectancy, by a large number of countries
 From HuffPo (and, The Atlantic, for that matter):
From HuffPo (and, The Atlantic, for that matter):
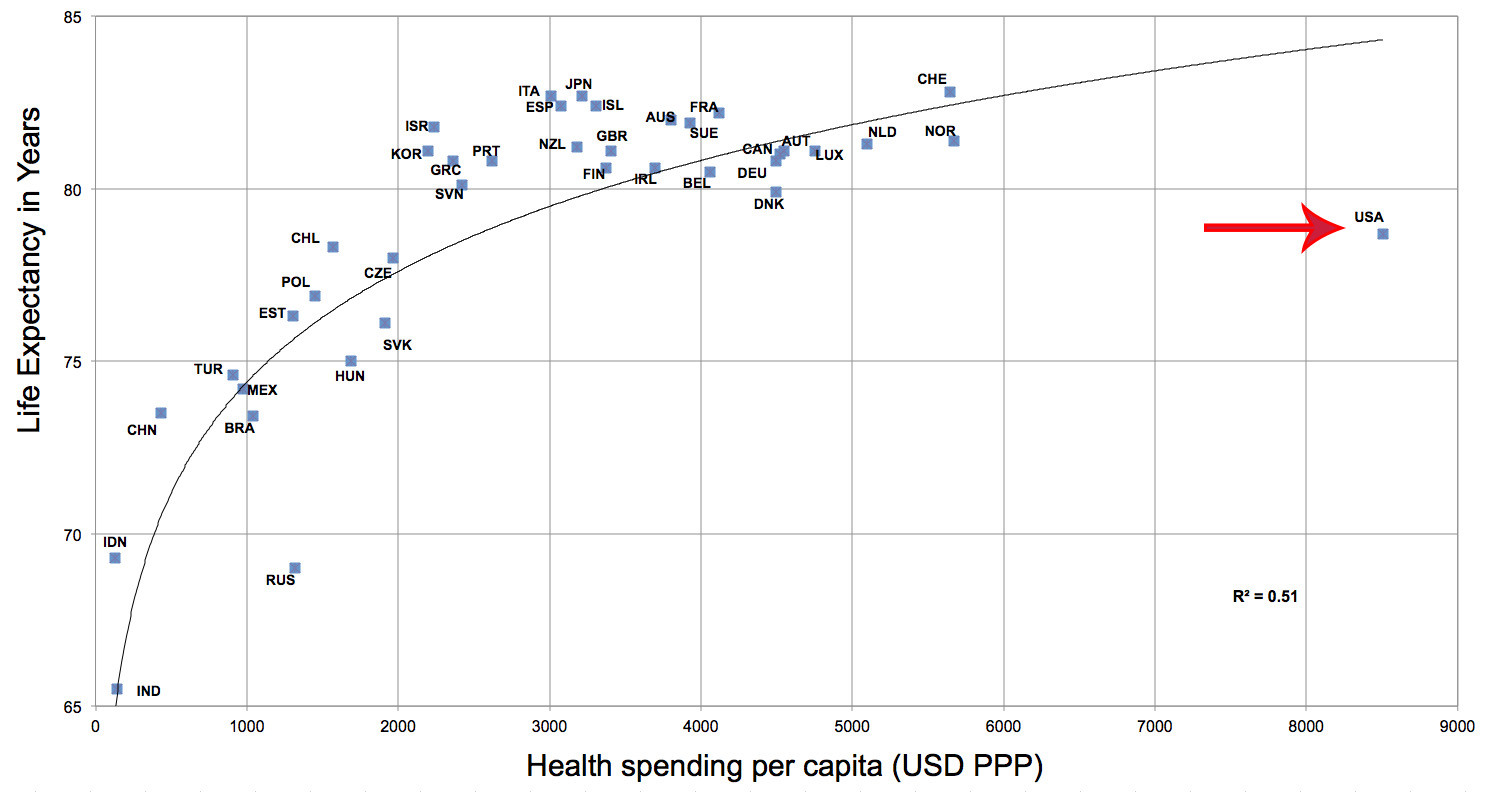
This graphs US per capita health spending per capita to life expectancy. The bottom line is this: we spend more per capita than any other country in the world and yet we are outperformed on a key metric, life expectancy, by a large number of countries. Indeed, as my co-authors and I note in our upcoming book, the US compares poorly with other democracies on a number of health indicators:
Not only is the US below the median in life expectancy and above the median in infant mortality rate and maternal mortality, it clusters with states that were classifiable as developing within the last two decades (or in some cases that still do): Brazil, Colombia, and Mexico are all in the second tier of the Human Development Index (i.e., “High Human Development”) and India and South Africa are in the third tier (“Medium Human Development”).
Note that our comparison is based on a smaller set of cases than is true of the graph above.* Indeed, the only health metric that we found that the US excelled at (so to speak) in our comparison set was obesity (we’re #1!).
Aaron Carroll (Professor of Pediatrics and Assistant Dean for Research Mentoring at Indiana University School of Medicine) has an interesting post concerning the graph above that is worth a read, which includes the following:
What bothers me most is not that we’re all the way on the right, or even that we are lower than we should be. It’s that we are all alone. We are spending so, so, so much more than everyone else. It’s not an even spread. I don’t want to get into arguments about the fit of the line, or about the fact that there’s a cutoff. It’s that those countries – representing lots more people than the US, by the way – are all in a reasonable relationship of more spending correlated with more life, to a point. Then there’s us. The difference is so large, it must be defended. It must be justified. What are we spending the money on, if not extending life?
Fair observations, I would say. The US’ position on the chart should, at least, raise questions. Carroll also has a post on the life expectancy metric itself (linked in the post linked above) that is worth reading as well.
Another metric worth a look, as linked from the HuffPo piece: Bloomberg’s health efficiency index. The US sits in a cluster with Turkey, Iran, Serbia, and Brazil. Countries that do better than the US include Mexico, China, and Colombia.
That there is something profoundly wrong with our system should be obvious. And, I would note, that the PPACA only deepens the flaws that lead to high per capita spending. Really, this is an area of policy where a more comparative understanding is needed. If huge chunks of the world are out-performing us, then perhaps we should look outward for solutions, yes?
And yes, I am aware that life expectancy alone is not the sina qua non of health stats (and some objections are addressed in the second Carroll post linked above–not to mention that we do poorly in other areas, comparatively speaking, as well). Still, the truly exceptional location of the US on the graph above should be enough to make one pause for thought.
*The countries in our study are as follows: Argentina, Australia, Austria, Belgium, Brazil, Canada, Chile, Colombia, Czech Republic, Denmark, Finland, France, Germany, Greece, Hungary, India, Israel, Italy, Japan, Korea, Mexico, Netherlands, New Zealand, Poland, Portugal, South Africa, Spain, Sweden, Switzerland, the United Kingdom, and the United States.
Greatest health care system in the world.
How many of those countries have a socialized form of healthcare service? I’m betting is most of them.
There are 2 major problems with the American Health Care system.
1. It’s a for profit enterprise.
2. The insurance industry has latched onto it like the blood sucking leaches they are.
@OzarkHillbilly:
* – the “cashectomy” performed better than any other nation.
@Vast Variety:
I’d guess than none are 100% socialized, without a private option. But I certainly expect that single payer frameworks, as a foundation, are common.
@john personna: Oh yeah. My wife is having a nerve induction study done today and $525 removed from her checking account. And we have “good” insurance.
However…just last week…Boehner called it the greatest Health Care System in the World.
Until a certain political party starts to recognize reality…facts….real reform can’t happen.
The PPACA is not perfect by any means…but it was what could be passed.
@C. Clavin: Anything could have been passed, the Democrats had a filibuster proof majority in the Senate and control of the House. Had they truly wanted single payer, they could have had it. But the problem was the folks who pay most of the Democrats bills (unions) don’t like single payer, and would have had a hissy fit.
@Bob Beller:
I am sure everyone will disagree with that, starting as it does from the false premise of a unified and far left Democratic Party.
@Bob Beller:
By the way Bob, are you calling for single-payer?
Or just making the irrational complaint that you should have been forced to a better solution over your own objections?
@Bob Beller:
Actually, this is untrue. There was only a relatively brief window during which the Dems had 60 votes in the Senate in mid 2009 until early 2010. Further, once Scott Brown win the Kennedy seat in Mass, the ability of the two chambers to negotiate a bill died and the House could only pass the Senate version, which was (for all practical purposes) a rough draft.
Although I agree the health care system is really bad we should not underestimate how the fact that Americans eat really badly impacts these numbers. Heavily processed foods are killing us. The frozen food section of my grocery store is as big as the produce section. In addition we get less exercise – we drive everywhere, in Europe they walk a lot more.
I think there are two problems here, one on each axis. There’s the costs and the life expectancy. We debate the first a lot, but we don’t really pay much attention to the second. I’d love to hear people’s opinions on how we can extend the average American lifespan.
it’s been well-knowv for a few years now: We spend 40% to 50% more per capita on health spending than the next most expensive countries (Norway and Switzerland), we fall short in many health indicators (life expectancy being one), and we still end up with over 15% of the population being uninsured.
To me a Single Payer system based on Switzerland’s model is the way to go – the system is not government run, it is only the base health insurance policy that is mandated by government, and the profit to the private insurance companies to offer the base policy is capped.
We’ll never get there. Conservatives are unhappy with the one socialized health program that we do have – Medicare – and would probably privatize it if they could.
American Exceptionalism (r)
We refuse to admit that we are getting the short end of the stick, because…
… ahhh…
mmmm…
hmmm.
(… unions are bad ? I dunno… what’s the talking point today, Chauncey? )
What are you writing about, Professor Taylor? I’d wager that if you controlled for wealth, you’d find that our Top Ten Percent have absolutely smashing life expectancy.
The Bottom 90, not so much.
And we have a political party singularly dedicated to increasing the income, health, and wealth gulf between the very well-off and the
helotspeasantsprolesReal Americans.And this is why we keep hearing/reading/seeing about why we should raise the Medicare and Social Security age. Because the executive suite can handle it.
First, we need to get over this irrational delusion as a nation that America=automatic Best in Everything For Freedom!(TM) and Everyone Else Is Doing It the Commie Way. Like they say, admitting is the first step towards recovery. You can’t have a meaningful discussion of deficiencies, possibilities and alternates if you can’t admit somebody’s doing it better then you.
Some places in the country need to take a deep calming breath and work on admitting out loud “America is not always Number One. That is OK because we need to work on that and we will”. Only then can we really start to solve these issues…..
@Pinky:
You could reduce poverty, for one. The babies of poor mothers die at birth more often than the babies of rich mothers. Poor people in general die younger because of lousy education and lousy access to health care. Fewer poor = longer lives.
Supply side: not enough doctors. Restrict supply, drive up prices. Look at physician compensation across the developed world. Our doctors are paid very, very well. It’s also true that medical school costs a lot of money (hey, look, another unjustifiably expensive but necessary fixture in our society!), but not enough to explain away the earnings gap. Not sure if the PPACA does anything about this.
Demand side: market failure (assymetry of information, fear-based decision-making, lack of sufficient cost controls in governmental programs). The PPACA helps address some of this, we think.
…
IIRC, the Dems had 60 votes for a total of something like 4 months (split into 2 periods). Even if they’d had 2 years, their caucus isn’t so unified as to be able to vote in lock-step like that. Lieberman (we hates him! We hates him Precious!) alone was enough to derail single-payer. And he wasn’t alone. There were enough moderate Dems (or D-Pharma, or whatever) to make sure that, absent crossover GOP votes (ha!) single-payer was not a realistic option. In a different universe, where Republicans weren’t completely unified against whatever liberals were for, updated daily, the whole thing probably shakes out differently (perhaps ala civil rights laws in the 60s, where you get bi-partisan votes that break down regionally).
@Rob in CT:
A little more than 4 months, but still not much in the grand scheme of things: July 7, 2009 to August 25, 2009, and then from September 25, 2009 to February 4, 2010.
@Ron Beasley:
We rely on processed food because we can reduce shopping and preparation time. Americans work very long hours, we live in suburbs where large grocery stores are the norm, and have large homes with large kitchens and large storage capacity.
Let’s say you’re a parent with two kids. You have a full time job which is likely more than 40 hours a week, plus commute times. You drive your kids to soccer, band, gymnastic class, a tutor, a sleep-over, and of course back and forth to the school which is nowhere near your home. Even if the school were near your home you wouldn’t let your kids walk because you’re paranoid about abduction. The school bus? That means getting the kids out of the house half an hour earlier than you already do, which is pretty damned tough because you barely get six hours of sleep as it is, and your kids were up til 2 AM doing pointless, rote homework so they’ll perform well on the stupid standardized test that determines local real estate prices.
So, guess what? You don’t really have the time it takes to clean and sort a bag of beans and soak them for a day and cook them for half a day. You have time to open a can or stick a package in the microwave.
@michael reynolds: Much of that does sound maddeningly familiar…
Sure, there are cultural factors in play here. Diet, excercise (lack of), sleep habits, and all that. That has to be part of the answer.
I suppose you could make this following argument (not sure I buy it):
We’re unhealthy because of diet and lifestyle, and we do the quintessentially American thing in response: throw shitloads of money at it, and get pissed when that doesn’t work.
😉
@michael reynolds:
The bit about walking to school made me cringe. I moved out into the country. Nice little town. Good school system. The elementary school is exactly 1 mile from my house. I do not fear abduction, but… no sidewalks. Between us and the school are relatively narrow, winding roads, including one kinda main road (that people, including me, often do 45+ on). I’m not worried about somebody snatching my daughters. I’m worried about them becoming roadkill. This, of course, is what you get when you move out to the country so you can have acres and acres of land.
Well, at least I do find time to cook nearly every meal myself. Success!
@michael reynolds: All that may be true but it doesn’t change the health impact of this chemistry set food.
It was interesting living in Italy for 8 months. Many or most Italians still cook meals, shop daily. They also don’t work and don’t have kids, and the kids they do have end up living at home until they’re 40.
The reason it’s hard to see what’s wrong with this picture… is because you’re looking at the small picture and missing the large one. If you take back, you will see a system that has, for the last several decades, been removing the nation’s resources from the vast majority of the people and appropriating them to the tiny handful on top. “We” made a decision that the only thing that mattered was profit, which of course accrues only to the owning class. And having come to that decision, we made everything else secondary. Wages had to be slashed so that wages could rise — and in order to make that happen, unions had to be essentially eliminated. Pensions had to be eliminated and their cash balances transferred to the owners. Public goods like parks, schools and roads had to be defunded so that taxes could be kept low on those who could afford to pay for them.
And of course, all politics had to be dominated by cash donations, so that the only ones who would be heard in government would be those could afford to pay. The Citizens United decision only formalized the system of “don’t pay don’t say.”
And so, sure, we have crappy health outcomes for everyone but the superrich. Because essentially no one in power in this country gives a damn except the tiny class of owners.
But we’re the greatest country in the world, so that’s all good.
@wr:
What you said.
Americans have been thoroughly brainwashed in the cult of money. People literally cannot conceive of any alternative to wealth as a value system. Politics is money, religion is money, art is money. Money money money and nothing but money.
Somewhere on my site there’s a bar chart illustrating the spending per age cohort as a percentage of total healthcare spending of several major economies including the United States. Only in the United States is healthcare spending so skewed towards people who are over age 65. In the others spending is much more evenly divided among the age cohorts.
It should go without saying that increased spending on individuals who are over 90 doesn’t do a lot to increase average life expectancy. Increased spending on people who are a lot younger might.
The usual claim is that the very high healthcare spending here on behalf of those 65 or older is because they have more health problems to treat. I’m not sure how you go about disambiguating that from our subsidizing the healthcare of the elderly so mightily.
Life expectency at birth is a bad proxy for health care, much less for evaluating a health care system. On should at a minimum, remove non-healthcare factors from life expectancy.
If you look, for instance, at life expectency at age 65, the US doesn’t do too bad, but still lags behind the major developed countries. The question is why?
A lot of people, including many commenters here, use life expectency to argue for single payer. Considering everyone over 65 in the US has access to a single-payer system, what does the US underperformance post-65 tell us? One could certainly make the claim that single-payer isn’t the ticket to better healthcare outcomes, but, like all such pat claims, that conclusion would have to be backed with some solid analysis. IMO, we really don’t know – there are any number of reasons, unrelated to the health care system, that could explain the disparity. Anyone making causal claims needs to show their work.
At the end of the day it really is hard to come to honest conclusions without a lot of caveats or without really digging deep into the various factors and establishing causality. It may be more useful for policy, and more meaningful with respect to improving outcomes, to look at specific areas where the US is doing well and where it isn’t. Examples – the US does not do well with respect to infant mortality, but does better than almost everyone when it comes to cancer survival. The relevant question, again, is why?
That said, I agree our system is broken and the PPACA doesn’t nothing to fix the underlying issues, much less live up to the grand promises of its strongest proponents.
@Steven L. Taylor: The point remains that the Democrats has the votes to pass anything they wanted – in theory. In reality, the Democratic caucus was divided and there were not enough votes for a public option, much less single payer. In short, the Democrats were unable to capitalize on their majority because of internal divisions between the moderate and progressive factions.
@michael reynolds: That sums it up. Don’t forget the wonderful institutional food our kids eat at school since we don’t have time to pack them proper lunches. All of which probably isn’t good for their long-term health and is something that won’t be addressed by whatever health-care system we happen to have.
@Andy: Except that it is a tad more complicated than that. And, moreover, demonstrates the difficulties of major legislation in our system. To pretend like it would have been an easy thing to vote major reform in those windows (and the inability after the window was closed to reconcile legislation between the two chambers) is to ignore how things work.
I am not saying more time would have brought single-payer, and it may not have produced anything better. However, to act like there conditions were optimal is just incorrect.
@Andy:
And while this is true (and it so noted in the post), just pointing this out does not (at all) deal with the comparative facts presented in the chart. Further, once we start throwing in a lot of other variables (some of which are mentioned in the post as well), one has to admit that we are not getting what we pay for.
@Steven L. Taylor: I’m not suggesting conditions were optimal and I never said that it would be “easy” to vote major reform in those windows – far from it.
@Andy: But even saying that Democrats could have passed “anything they wanted” ignore the fact that they were denied even the chance to reconcile the House and Senate versions, and had to go with the Senate version or get nothing, The amount of time present didn’t even allow for normal legislative activity. And since the super-majority in the Senate did not materialize until late in the year (a combo of Specter’s switch and the Minnesota race being settled) there was a lot of time to know that the votes would be available.
It is an incorrect talking point to act as if the Dems had a true, legit chance to pass whatever they wanted. That would have taken at least a full two year term with a Congress that had 60 votes in the Senate.
I’d like to cross-culturally compare life expectancy at, say, 40 with life expectancy at 65. My hunch is that it’s the “gap decades” – when your body starts to go wrong on you but Americans disproportionately lack adequate health coverage – that provide a winnowing effect. Or, as a cross-cultural comparison, what percentage of each country’s 40-year-olds reach 65?
@Steven L. Taylor:
What do you mean by “deal with the comparative facts in the chart?” What, exactly, are we supposed to deal with?
The “facts” as presented are misleading and, at best, tell us something we already know – which is that we are not getting good value for our money.
@Andy: Simply the reason for then discrepancy over 65 is that despite the fact that they now have access to decent medical care, huge swaths of them did not for the previous 65. Because of this when they finally get Medicare and actually seek treatment they have let their problems fester for years (if not decades). This is the reason why increasing Medicare age is shown to increase costs because because it just leads to sicker people when they finally get it.
@Andy:
You are contesting that there is a cluster of countries with higher life expectancy than the US? (As well as better performance on a number of variables?).
You are contesting that the US spends far more per capita on health care than, well, anybody?
Although, really, you do accept both, so I am not sure why you put facts in scare quotes. Further, we agree that we are not getting value for our money. So why are you dismissive of the chart?
@Pinky:
I was just out on a hike with the kid and the dog .. I saw a lot of people I’d judge to have good expectancy.
That we could finish with a jog made me feel about my old self.
@Steven L. Taylor: Ok, so the argument is the Democrats couldn’t pass whatever they wanted because they didn’t have enough time to take advantage of the super-majority? Again, I think this is incorrect – the problem was division in the Democratic caucus regarding the specifics in the PPACA which made the “legislative process” last much longer than normal. The reason it took so long was because there wasn’t consensus in the Democratic party over the the details of what became the PPACA. The House didn’t pass it’s bill until early November and even then it barely passed.
The point here is that the Democrats did have the opportunity to pass “whatever they wanted.” The problem was not one of time, the problem was that Democrats could not agree on what “they wanted.”
One should also consider the opportunity costs – the internal debate over the PPACA took so much time and energy that the Democrats weren’t able to use the supermajority to pass other types of legislation, a point which has been made before.
“Made me feel [good] about my old self.” Whether that made up for last night’s whole hog and drinks is another question.
Re. Complaints about this graph, got a better one? Because dislike of data is not a strong argument.
@Andy:
That sir, is a manufactured history.
None of us are so young that we do not remember the compromises of the bill.
I mean, given all that legislative power, where is the public option?
Clearly, the U.S. needs to invest more money in healthcare.
@Steven L. Taylor: I’m dismissive of the chart for reasons I’ve already stated – namely life expectency is a poor proxy for health care, particularly when compared to health care spending. Because, again, there are a lot of non-trival factors that determine life expectancy that have absolutely nothing to do with health care much less the amount of money spent on health care. So the comparison is misleading and implies there is a some kind of direct relationship between the two. Just look at many of the comments about the chart here – a lot of people think the relationship is not only direct, but is causal.
@James:
Please cite some evidence for this assertion.
@Andy:
Prof. Taylor is right, you’re wrong. It’s absurd to argue that Democrats had a realistic chance to create and then pass one of the most complex pieces of legislation imaginable in two 2-month windows. It ignores the realities of politics. Yes, there was some dissent in the Democratic caucus, but that doesn’t alter the underlying political realities, and it ignores the fact that Mr. Obama was straining every nerve to get some support from Republicans who were determined to oppose absolutely everything, even a health care plan that was a virtual Xerox copy of that passed by their own presidential nominee.
We got what we could get given the fact that Republicans retired from actual governance so they could focus on race-baiting and conspiracy-mongering.
As I’ve said many times over at Dave’s place what we achieved was to move the debate from the Republican position which was “Screw the poor, screw working people, definitely screw minorities, keep everything right where it is despite the fact that the system is going off a cliff.” It required this much effort, and this much expense, and this flawed system just to break the Republican fantasy that everything was fine, just fine, and would be even better if poor people would just die.
It’s the price we pay for having one party devoted to resentment, hate, ignorance and greed. We drag you people along like a ball and chain and then you actually have the nerve to ask why we aren’t running faster. We’re weighed down by cretins, that’s why.
@john personna:
Perhaps you missed what i’ve repeatedly said – namely the divsion in the Democratic party. There was no public option because there wasn’t enough support for it in the Democratic caucus.
The medicine we all seek is not in a bottle but in lifestyle. You think decades of 40+ hours of work per week with 2 weeks (maybe) of time off is healthy? Decades of constant wondering of how this or that is going to be paid for translates into physical stress on the body. Throw in a liberal amount of constant uncertainty about employment and the body simply will not function optimally in such a hyper-worrisome environment.
People in other countries have a completely different attitude towards work than Americans do and the mental freedom that “laziness” attitude provides translates into more happiness and satisfaction than what is experienced in this country..even though it yields less material wealth. Keep in mind that this is all relative, the Japanese live longer even though their attitude towards work is much more stringent than ours. They seem to derive some sense of satisfaction from this lifestyle though. No one would argue that Americans derive mental and emotions stimulation from work culture. They derive satisfaction from the things money provides but not necessarily the hoops jumped to get the money. 25 days plus weekends per year to pursue the things one enjoys?!?!? Who’d eat at that buffet?
@michael reynolds:
Well, the legislation didn’t have to be one of the most complex pieces of legislation imaginable. Why do you think it was so complex? Because of the “realities of politics” and those realities included a Democratic caucus that was not united regarding the specifics of the legislation. So a lot of stuff had to be added to satisfy all the various interests involved to get sufficient votes.
Again, I think people are missing my point here. It is a fact that the Democrats had a supermajority where they could have, in theory, passed anything they wanted. No one can deny the vote math. Key point is “in theory,” which I put in my original comment. Let me say it again – “IN THEORY.” In practice they could not capitalize on the supermajority because they lacked internal cohesion on the topic of health care reform. I’m not sure what is controversial about the fact that Democrats are/were not completely united on health reform policy.
Furthermore, I’ve never suggested there was some “magic” health reform bill that would have united all Democrats and allowed them to utilized that supermajority.
@Andy:http://www.census.gov/hhes/www/hlthins/data/incpovhlth/2012/tables.html 15% of Americans are uninsured
http://content.healthaffairs.org/cgi/reprint/hlthaff.27.4.w298v1?ijkey=rhRn2Tr4HAKZ.&keytype=ref&siteid=healthaff 42% of US adults uninsured or underinsured.
@Andy:
In short, even thought there might have been, for a relatively short time, 60 Democrats in the Senate, there were never 60 votes for the public option. Ironically, now that the filibuster has been essentially killed, if the Democrats controlled the House, they probably could pass at least a public option … even if the few remaining “conservative” Democrats chose to vote against it. So in a way you’re kind of right. If the Democrats had simply abolished the filibuster 4 years sooner, then they really could have passed almost any type of health care reform they wanted to.
Oh but wait, passing legislation with a simple majority would have been
unconstitutionalsomething every Conservative would have screamed about for years to come. (kind of like they’re still doing about the crappy compromise PPACA bill that did pass)@wr: Wow, what a bunch of typos and wrong words in that message. My thanks to those who were able to read and make sense of it. No more typing until the jet lag’s over!
@James:
Can you demonstrate that a lack of insurance or underinsurance (however that is defined) has any relationship at all to to longevity after age 65? If there is a relationship, is it causal?
@Andy:
Your position is contradictory isn’t it? With an internal consistency problem?
You say both that the Democrats had internal division AND could pass whatever they wanted.
Which is it?
Really Andy, you might be doing a shade better than the others, but you are arguing from the same position … that is, an imagined counter-factual that makes your argument work.
Shorter Critics Above:
Democrats could have done better, because I can imagine a world where they did better.
This while of course, Republicans volunteer and have responsibility for jack shit.
To add to the discussion, part of the point I was trying to make to Andy (and in general) was that time constraints that existed in this case curtailed the ability of various factions of Democrats to negotiate. There was, ultimately, only very limited inter-chamber negotiation. Had their been a full congress (2 years) to deal with the legislation, there would have been more negotiations.
@Andy: http://jama.jamanetwork.com/article.aspx?articleid=193207
@john personna: Where is the contradiction? Is the distinction between what is theoretically possible and what is realistically/politically possible so hard to grasp? Is it really news to anyone that there was a conflict between progressive and moderate Democrats that impacted the PPACA and the legislative process (to include how long that process took)?
But this is really a minor point, a side issue to the main point of the post.
@James: That survey doesn’t address the question, much less answer it. Your quoted portion only suggests that costs to medicare may be higher – it, and the unquoted portions, do not make any claims or guesses about life expectancy after 65, much less provide substantive evidence.
Just to be clear, because, after all, this is the OTB comment section, I’m not saying one way or another that uninsured do or do not affect life expectancy after 65 – I honestly don’t know. But if someone is going to claim that the uninsured is what accounts for the discrepancy between the US and other developed nations, as opposed to other potential factors, then one needs to provide evidence to that effect. If such evidence exists, I would like to see it.
@Andy:
This is what I was replying to:
I see a contradiction here, I mean in one line, really. That scecond line starts “the Democrats did have the opportunity to pass whatever they wanted” and ends that they “could not agree on what they wanted.”
That sir, is a contradiction (and a misreading of history).
As an alternate history, consider that “the Democrats passed what they could.”
And that there were all sorts of things they could not have passed.
Also, this sentence fights it self pretty well:
Basically, long story short, if you believe that there are “non-healthcare factors” making us sick and/or die young, get out in front of them. Name them and a plan to deal with them.
IOW when someone is saying that we have a broken system, because we spend more than anyone and still die sooner than most … I really think you should agree, rather than deflect at that point.
Because when you deflect you are basically defending the status quo while (contradiction) blaming its failure on “non-healthcare factors”.
@john personnaPerhaps the quoted portion was poorly worded on my part, hopefully my point is now clarified.
@John personna
On the first point, you should go back and reread what I actually wrote – I agreed we have a broken system and I agreed we spend more than anyone else and are getting poor value for our money. I also pointed out that even when one considers life expectancy from 65, we Americans still “die sooner.” I can agree with all of that and still argue the chart is misleading and point out the flaws of using life expectancy from birth as a proxy for health care.
Secondly, if you go back and read anything I’ve ever written on the topic here or anywhere else, you’ll find that I am about as far away from being a defender of the “status quo” as one can be on this subject.
BTW, I’m not sure why the editor bolded a portion of your quote – it was unintentional and I can’t seem to get rid of it.
@Andy:
As has been said, two months twice is not enough time for a divided caucus to negotiate getting ‘anything they want’.
More importantly, life expectancy vs health care costs from birth is not a good (and certainly not a complete) comparison between any two nations. However when you look at all OECD nations many, if not most, of those confounding factors start to matter less. Germany in nearly as obese as the US while smoking more (virtually all of Europe smokes more than we do). Northern European nations tend to smoke and drink more.
You mentioned early that the US is closer to those other OECD nations when only looking at 65+ yr olds. For some reason you seem to think this supports the notion that moving to socialized medicine is not effective in increasing life expectancy. Why is that? That fact seems to run counter to your overall argument rather than supporting it.
@Todd:
The filibuster has only been removed as an option for certain nominations. The filibuster is still available to delay or derail normal legislation.
@Andy:
Again, I think people are missing my point here.
If so, that’s your fault.
@Andy: What I linked to showed precisely what I claimed. Not having access to good medical care is correlated with worse patient outcomes, particularly with chronic disease. Giving people access to medical care to people at 65 doesn’t magically fix all the years their illnesses went untreated. This isn’t novel or, at least in the medical community, controversial. Not understanding the evidence does not change it.
@Grewgills:
I understand that this rule change only affected executive appointments and non-Supreme Court judicial nominations. But let’s be real … for all intents and purposes the filibuster is dead.
The minority party will no longer be able to stop something that at least 51 Senators really want to pass … even if ultimately getting it passed means they have to vote again to change the filibuster rules on legislation. Same thing if President Obama has the opportunity to nominate another Justice (or two) to the Supreme Court. If the majority of rational people (i.e. not Conservatives) deem the nominee to be relatively mainstream, and more than 50 Senators indicate that they would vote to confirm, do you really think the Republicans would be able to sustain a filibuster?
… and if Republicans get control of the Senate in 2014, the whole filibuster will be gone anyway … they’re going to want to make President Obama veto as many potentially “embarrassing” bills as possible during his last two years in office.
If memory serves, average miles driven per year accounts for some of the higher US mortality rate.
@Grewgills:
Here is what I wrote (emphasis added) :
So, your characterization that I support the notion that moving to socialized medicine is not effective in increasing life expectancy is not accurate. I’m don’t know the answer, I’m simply skeptical of the superficial claims that get tossed about. Single payer is often asserted as the key factor that makes other systems superior to ours, but the causal relationships are weak – in other words, are the benefits in other countries because of due to single payer or are they due to other factors?
And here’s why I’m skeptical. Take a look at this chart. We have a single payer system for the elderly in this country and right now that system is not giving us worse outcomes than comparable developed countries (in terms of life expectancy) despite spending 2-8 times the money as those countries. What does that tell us? If single payer and/or “Medicare for all” is such a great system, then why does it underperform and cost so much more than other countries? This is a question that advocates of single payer need to answer.
I don’t know the answer, but my suspicion is that costs and health outcomes aren’t all that dependent on the system of coverage. I suspect that other, unrelated factors, account for the difference.
@James:
Here’s what you originally wrote:
The statement in your most recent comment I agree with – yes, people who don’t have access to medical care have worse patient outcomes. That is pretty well demonstrated in the literature. However, that was not your original claim and life expectancy for the 65+ cohort is a completely different question. You suggested the discrepancy between the US and other developed countries was due to lack of care earlier in life, but you’ve provided nothing to show that is at all a factor and, if it is, how big a factor it is.
@michael reynolds: plus, poor people kill each other more often…..get real. the countries ahead of us are not as diverse “ethnically”. do the math, we’re “free” to live and die how we want to- or sometimes are just innocent victims.
@Pinky: good one, we’re also free to kill each other with cars!
@Andy:
You have admitted that overall health outcomes, at least re life expectancy, are worse for the US relative to other OECD nations. You have also said that the 65+ cohort in the US is NOT experiencing worse outcomes than other OECD nations (that have universal care, often single payer). That the negative relative health outcomes, by your own account, seem to even out between the US and other OECD nations when we switch to single payer (65+), tends to support the notion that single payer healthcare improves health outcomes.
That we manage to pay more for it than anyone else has a variety of reasons, not least of which is supply. Look at relative numbers of doctors per 100K in the US and Western Europe, Canada, and Japan. Other potential reasons have been covered, including substandard care for a substantial cohort (~15%) prior to acquiring Medicare. No population comparisons are simple, but when you have over 30 countries holding pretty tight around an asymptotic curve and we are the one LARGE outlier, then something is going on. Look at those other countries. What major differences between us and all of those other countries do you see?
@bill:
Why the scare quotes around “ethnically”?
With just a quick look I see Mexico and Brazil. Do you want to try and argue that Brazil is less ethnically diverse than the US?
@Grewgills:
That was a typo on my part. I meant to say “system is giving us worse outcomes than comparable developed countries.” Sorry for the error.
First, they don’t “even out.” The US still lags behind, it just doesn’t lag behind as much. Secondly, you speculate that the reason the gap is smaller is due to single payer, but that’s just speculation. There are many other potential factors and some of them we’ve already discussed, such as a lower level of accidents and violent death, exclusion of infant mortality, etc. There are undoubtedly other factors we haven’t considered.
Given the potential factors involved, one simply can’t assume that one factor is responsible without some clear evidence demonstrating the factor is relevant.
Ok, I generally agree with your list of reasons, but that kind of reinforces my point – there are a lot of factors besides whether a country is single-payer or not that determine costs and outcomes.
This could be a long list, but here are what I think are a couple of the major factors:
Political/social cohesion. The US is a lot more diverse than most other countries. We are a political union and not a nation state. It’s therefore easier for most other nations to make tough decisions regarding things like health care spending (This is something we are not currently capable of.). Consensus on social welfare is easier. Nations-states generally have a much stronger social compact than we do. We are federal system with a central government with limited power, etc.
Scale – we’re simply much bigger in terms of land area and population than most of these other countries. Solutions that working in a country of 5 million won’t necessarily scale up to work in a country of 320 million. Access to medical care is more limited because of geography – our population is more spread out, exacerbating our doctor shortage.
There are some others, but it’s midnight and I’m tired and need to go to bed. Think I’m done with this thread, have the last word. Thanks for the debate.
@Andy: Poor, poor inarticulate Andy. You obviously are thinking about this very hard and finding it hard to speak clearly. Just as an example, you say that the US is “…political union not a nation state.” Well, we all know what you are trying to get to — the problems with the unequal access to the offered health insurance policies because the states have the right to set up exchanges or not, to expand medicaid or not and so on. But the rather startling pronouncement that the United States of America is not a nation state raises so many hackles that it’s hard to get to the kernel inside the nut.
This business of ‘the Democrats had majorities’ so why didn’t they just pass the dang thing? Well, because life is complicated. If possessing congressional majorities is enough, why didn’t we have HillaryCare? After all, the 103d Congress had bilateral Dem majorities.
Pretty simple answer: Because the health insurance industry fought desperately to defeat the reform of their business in ’93. Why do we have ObamaCare, then? Because the health insurance industry got to shape the content of the PPACA and fought FOR it in ’09. The final tally was what it was because of the waverers at the margins (Sen Ben Nelson, Sen Grassley). And that’s how our politics works; on close votes the power lies in the hands of the marginal congressmen.
On the Original Question: Bad health outcomes for hugely expensive health investment. I once asked this question to a group of foreign MDs who were here on fellowships studying Trauma Medicine. (I’m an ICU Nurse who’s worked many years in NeuroTrauma at 2 academic hospitals with level 1 Trauma Centers.) These guys/gals worked parttime as ER docs at smaller local hospitals and studied/performed surgery at the University Hospital. They were unanimous that the difference was medical care of chronic diseases. In England, Germany, Taiwan, Switzerland and several other countries people with diabetes or COPD or who are pregant have their conditions handled by local ‘PMPs’ (primary medical providers) and almost never show up with advanced states of deterioration. The result is that the very very expensive business of making my professional acquaintance is a very rare thing. And a much smaller number of premature births. And so on.
@Andy:
It is true that the US still lags when we look at older populations. However, the numbers do coverage far more with other OECD countries. While not proof in and of itself, that bit of evidence supports the hypothesis that universal care improves life expectancy and it may be that the convergence suggests that perhaps the difference pre-Medicare (and why there is a gap) is because of the lack of universal care contributes to the gap in the first place. The gap is not going to be fixed the day all Americans turn 65 and then have Medicare.
BTW, you are conflating “single-payer” (which is one option) with a truly “universal health care system.” Not all universal systems use single payer. Canada is single-payer, Germany is not. The UK has the National Health Service, wherein the government owns and provides health care (which is not single-payer the way that Canada’s system, or Medicare is).
@Andy:
Well, I love the chart, because it combines two available and reliable numbers: the reporting for costs and for life expectancy. Costs are certainly real, and life expectancy has certainly proven a good proxy for both health and healthcare around the world. That is, to score high on life expectancy you need BOTH good health and health care.
I also suspect that we could send much less, with a National Health which is “worse” in some regard (those dreaded two-week delays to see a specialist) and still have about the same life expectancy. Why? Because that’s the way the Czechs are doing it. While spending 1/4 as much as we do.
Now … don’t tell me that is because Czechs are inherently 4x healthier, to start with, than Americans.
@Andy:
You are conflating variables. Size of population and size of territory are different variables.
I would note that pop size is at least partially controlled for in one of the variables we are discussing: spending is per capita.
I would note that Japan has a pretty big population (~128 million). Granted, that is less than half the size of the US pop, but it isn’t 5 million, either.
Australia is pretty big territory-wise, but they are going better than we are.
I can see an argument that size of territory leads to a difficulty in evenly providing services. However, given that most American live in urban areas, I am not sure that dispersal is an adequate answer to the problem.
(Or to put it differently, the cashectomy doesn’t always change the patient outcome by that much.)
@Andy:
BTW: same is true of Germany. It came together from a variety of independent units (that were, in fact, more independent from one another than the US states ever were) and yet they make it work.
Belgium, Spain, and Canada have more complicated diversity problems than does the Unites States. Likewise, they outperform.
BTW: do you know what the main thing that truly differentiates the US from all of the advanced economies on that graph? Policy-making (and implementation) is harder here than in any of those other places.
Found on the internets:
@Andy:
Actually while bigger in terms of land area can be a problem when that means lower population density (the northern territories in Canada can tell you all the problems that come with that scenario), having a bigger population in itself scales very well – in fact gives you increased efficiency because it makes it more cost effective to buy some of the more rarely used but very expensive pieces of equipment and specialists.
And in terms of size, countries such as Canada and Austrialia have roughly the same geographical extent with a much smaller population, so America is hardly unique in dealing with that.
@Andy:
So when we switch to universal care our health outcomes move closer to all of those other nations, which also happen to have universal care. That is interesting isn’t it. Why do you think that is so?
We were born a political union, but we are now and have been for more than half our history a nation state. If you want to make a comparison with a real political union, then compare the US to the EU as a whole. All of the EU nations have managed to implement universal care and the overall the cost/benefit equation works out in their favor.
The US is more diverse than SOME of those other nations. Steven has pointed out a couple of countries that have greater ethnic diversity and or social cohesion than the US, I would add Brazil to his list.
@Steven L. Taylor:
and
@Grewgills:
It’s simply correlation. Both of you strongly imply that single payer/universal coverage system is the reason, yet all you can point to is one correlation while ignoring other possibilities and other correlations.
For example, one could argue that the reason the gap closes is because we spend 2-8 times as much money on our 65+ population than any other country. That correlation is just as “valid” as what you mentioned and it’s jus as evidence free. We can argue correlations all day, but that gets nowhere. We don’t know the truth without digging deeper and if we are honest with ourselves we should not leap to conclusions about cause and effect based on a correlation that happens to agree with what we already believe. If you really believe the system is responsible, then let’s see some evidence. I, for one, will remain skeptical of any theory until I see more that correlation.
@Steven L. Taylor:
Yes, that was a key difference I was getting at when I mentioned political cohesion. We are a political union and not a nation-state. Government power is much more decentralized here than any comparable developed country. Our system is not designed to make solutions at the federal level easy. Our states aren’t mere administrative units as they are in other countries – they have a non-trivial amount of protected soveriegnty. We don’t have a parliamentary political system. All these things make national level policymaking more difficult. That is a factor we can’t ignore in examining solutions that will work for us.
@Grewgills: I wanted to address something in response to this earlier comment:
If you look at the data, we somewhat more per capita than other countries for people under age 60. As I noted earlier, we may mutliples more (2-8x) for people over age 60. So our health spending is concentrated on the old cohort and we spend so much there that it pushes our per capita average for the entire population way up. This is another way the chart in the original post is misleading.
So, while I agree with the items you listed in a general sense, I don’t think they can explain why spending on the over-60 age group is dramatically higher than the under-50 age group AND dramatically higher than any other country.
@Andy:
Yes, but it is correlation that has a logical basis for potential correlation. No one is saying that this proves anything, but it does lead to a series of worthwhile questions.
Further, the change in comparative life expectancy once US citizens head into Medicate is suggestive of causation (although, again, not proof thereof).
While it is true that correlation does not prove causation, but correlation suggests the need for further inquiry, especially since that there is a logical basis for assuming that how much is spent should matter.
@Andy:
The difficulties in policy-making are not because “political union” v, “nation-state” (terms which you really aren’t using properly, btw). The issue is that it takes three distinction political actors (House, Senate, and Pres) to make policy and the Senate not only over-represents small populations, but it works under super-majority rules.
@Andy:
This is true in Belgium, Canada, Germany, and Switzerland, to name four cases that do better in this area than do we.
@Andy:
I do agree, and basically say so in a different way above, that our presidential system is part of the issue. This is far more the issue than your political union/nation-state dichotomy (because, again, there are plenty of federal systems that have universal health care).
@Andy:
That’s a myth. Most of the US population lives in densely concentrated urban/surburban areas, making us less, not more, spread out than the rest of the world. We do have vast empty tracts of land, but nobody really lives there, so we don’t have to provide many doctors for those areas. Per Wikipedia:
It [the USA] is very urbanized, with 82% residing in cities and suburbs as of 2008 (the worldwide urban rate is 50.5%[3]).
Probably if you want to boil it done to basics, the US system impedes policy-making, which favors conservative solutions (in the true sense of the word). Conservative solutions favor entrenched elites over the mass population. As a result, we get inefficient systems that favor wealthier citizens who do not want to pay higher taxes. The lower class/lower middle classes get the poorest care (as is reflected in the Red State/Blue States business)
(This is the blog comment version of a far larger point).
This isn’t unique to the US, but is also true of many other countries such as Canada, Germany, the UK, Spain, Switzerland, Belgium, etc., all of which have better health outcomes than we do.
@Steven L. Taylor: Put another way, Americans often think that federalism is what makes us different, but that is not the case. Again, lots of federal systems, some of which arguably give their states more power in some ways than is the case in the US.
What makes our federalism different is the combination of co-equality in Senate representation with wildly divergent populations in the states coupled with the filibuster rule. It isn’t federalism that is the issue, it is the structure and functioning of the Senate.
Gosh, that took an amazing turn! Went from health care costs to civics lesson. Pretty cool.
@Andy:
What the heck have you proven here, Andy?
That you can ignore a chart, and spout unsupported theories in opposition?
What do you really want to say, that we have high health care costs because we are obese?
There are studies for that:
“4 percent” does not fix our problem.
@ Rafer Janders
Hey, no fair using facts 🙂